The Largest Medicaid Cut in History
WASHINGTON, D.C. — On July 4, 2025, President Donald Trump signed the One Big Beautiful Bill Act into law. The sweeping legislation, passed by the House 218–214 and the Senate 51–50 with Vice President Vance casting the tie-breaking vote, includes approximately $1 trillion in cuts to federal Medicaid spending over 10 years—the largest reduction to the program since its creation in 1965. The cuts are designed to partially offset trillions of dollars in extended tax cuts from the 2017 Tax Cuts and Jobs Act.
The Congressional Budget Office projects that the cuts will result in 11.8 million individuals directly losing their Medicaid health insurance coverage, with an additional 3.1 million people losing Medicaid-funded marketplace plan coverage. The American Psychological Association estimates the federal funding reduction at 15 percent. The magnitude of the cut is unprecedented and, according to disability advocates, will lead to millions losing health insurance, significant regression in Medicaid services, and the elimination of some Medicaid programs entirely.
Maria Town, president and CEO of the American Association of People with Disabilities, called the law’s passage a devastating day for disabled Americans, stating that the catastrophic effects of the bill will reverberate for generations. The Autism Society of America issued a statement expressing deep concern about the impact on autistic individuals and their families, noting that Medicaid funds essential services including ABA therapy, speech therapy, occupational therapy, and home and community-based supports that enable autistic people to live in their communities.
The One Big Beautiful Bill Act represents the most significant rollback of the social safety net since the 1990s welfare reform. The $1 trillion in Medicaid cuts alone exceeds the entire annual budget of most federal agencies.
HCBS: The First Services on the Chopping Block
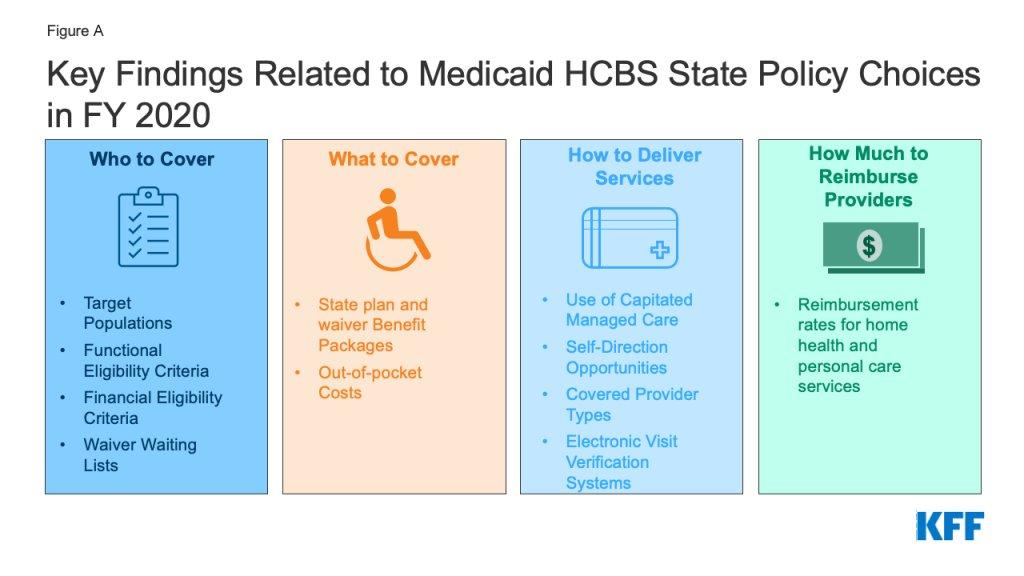
Disability advocates have been warning for months that there is no way to insulate people with disabilities from Medicaid cuts of this magnitude. Their particular concern is home and community-based services, or HCBS—the optional Medicaid offerings that fund personal care aides, supported employment, adult day programs, residential support, and other services that enable people with disabilities to live in their communities rather than in institutions.
Zoe Gross, director of advocacy at the Autistic Self Advocacy Network, told Disability Scoop that because states are not required to provide HCBS to everyone who needs them, states faced with a huge loss of federal funding for Medicaid will cut HCBS first. She warned that this will lead to disabled people going without lifeline services like assistance with eating, dressing, using the bathroom, going to work, and other activities of daily living.
Research from the Center for American Progress confirms this pattern: when federal funding for Medicaid decreases, states tend to cut optional benefits—including HCBS—first. It is nearly impossible to carve out a specific population, such as disabled people or elderly people, because the cuts affect everyone through hospital closures, workforce reductions, and across-the-board service contractions. Advocates note that 86 percent of optional Medicaid spending funds services for disabled and elderly Americans, making these populations disproportionately exposed to any reduction in optional services.
Kim Musheno, senior director of Medicaid policy at The Arc of the United States, described the situation as a convergence of pressures that threatens to erase years of progress and force more people with disabilities and older adults into institutional settings. She cited unprecedented federal threats to HCBS under the guise of fraud, waste, and abuse, combined with historic Medicaid cuts and rising demand for services, as posing an existential threat to an already fragile developmental disability services system.
The Work Requirements Problem
The OBBBA imposes work requirements on most Medicaid expansion enrollees, requiring 80 hours per month of work, volunteering, or work-related activity as a condition of maintaining coverage. While the law provides exemptions for individuals who are medically frail—including those with disabling mental disorders—the administrative burden of documenting exempt status creates a significant barrier for people with disabilities who qualify for exemptions but may struggle with the paperwork required to prove it.
When Arkansas implemented a similar work requirement under a previous waiver, thousands of people lost coverage due to paperwork problems and reporting errors—not because they stopped working or ceased to be eligible. The policy particularly affects the 2.6 million adults with disabilities who receive Medicaid but do not qualify for federal disability benefits. These individuals often cannot work consistently due to health conditions but are not automatically exempt from work requirements under the OBBBA framework.
For autistic adults, the work requirement creates a specific risk. Many autistic adults receive Medicaid-funded services that support their employment, daily living, and community participation. If administrative barriers cause them to lose Medicaid coverage—even temporarily—they lose access to the very services that enable them to maintain the work activity that the law requires. The circular logic of the requirement is not lost on disability advocates: cutting the services that enable work as a consequence of failing to demonstrate work.
The ABA-Specific Impact
For the ABA industry specifically, the OBBBA Medicaid cuts represent the most significant federal policy threat the sector has faced. Medicaid is the single largest payer for ABA services in many states, and Trilliant Health data show that Medicaid-covered ABA volume grew 298 percent from 2019 to 2024. Any reduction in Medicaid funding for ABA—whether through direct rate cuts, reduced authorized hours, tighter eligibility, or administrative barriers—will hit the revenue base of ABA providers directly.
The state-level Medicaid actions that have already occurred—Nebraska’s 48 percent rate cut, Indiana’s lifetime hour caps, Colorado and North Carolina’s proposed funding reductions—foreshadow what could happen at a much larger scale as states absorb the federal funding reduction. The OBBBA provisions take effect in stages: some restrictions became effective immediately upon enactment, enhanced federal matching for expansion states sunsets in January 2026, eligibility narrowing for non-citizens takes effect in October 2026, and work requirements begin in January 2027.
Dexter Braff, president of The Braff Group, noted at BHB’s INVEST conference that with most OBBBA provisions not going into effect until 2027, Medicaid unknowns will continue to shadow behavioral health M&A. Buyers like certainty, and no one knows the real impact until the provisions take effect. The uncertainty is already affecting deal activity: investors are holding their finances close and watching the situation develop before committing capital to ABA acquisitions that depend on Medicaid revenue.
The combination of federal Medicaid cuts, state-level rate reductions, intensified payer scrutiny, and the transition to outcomes-based reimbursement creates a multi-front challenge for ABA providers that is qualitatively different from anything the industry has faced. Previous challenges—workforce shortages, RBT turnover, PE consolidation concerns—were structural but manageable. A $1 trillion Medicaid reduction is a macroeconomic force that no individual provider can manage through operational improvement alone.
What Comes Next
Several states are already weighing proposals to reduce HCBS funding in anticipation of the federal cuts. Idaho, Missouri, Maryland, Colorado, Utah, and Washington are among the states considering HCBS budget reductions, citing financial pressure as they brace for the OBBBA impact. At the federal level, the Trump administration has targeted Medicaid as part of a broader effort to weed out fraud, with CMS threatening to withhold billions from states over HCBS program growth that the agency characterizes as suspicious.
Disability advocates push back on the fraud framing. Alison Barkoff, a health law professor at George Washington University, noted that growth in HCBS is a result of decades of bipartisan federal and state efforts to rebalance funding from institutional care to community-based care. Characterizing that growth as fraud ignores the policy history and the Supreme Court’s Olmstead decision, which established that unnecessary institutionalization of people with disabilities violates the Americans with Disabilities Act.
For ABA providers, the immediate practical imperative is to diversify payer mix away from Medicaid dependence where possible, build relationships with commercial payers, demonstrate outcomes data that justifies continued coverage, and invest in the operational efficiency and technology infrastructure needed to deliver services at lower reimbursement rates. Providers whose revenue is predominantly Medicaid-funded and who cannot demonstrate measurable outcomes are the most vulnerable to the cuts that are coming.
The One Big Beautiful Bill Act is not a state-level rate adjustment that can be absorbed through operational tightening. It is a structural reduction in the federal government’s commitment to Medicaid-funded healthcare services for vulnerable populations. For the ABA industry, it means that the funding infrastructure that enabled the sector’s explosive growth—the very Medicaid expansion and mandate framework that parent advocates fought for over two decades—is being systematically dismantled. The autism community won the coverage fight. The question now is whether it can survive the funding fight that follows.
AT A GLANCE
| Law: | One Big Beautiful Bill Act (H.R. 1); signed July 4, 2025 |
| Medicaid cuts: | ~$1.02 trillion over 10 years (CBO); largest in program history |
| Coverage loss: | 11.8M directly + 3.1M marketplace = ~14.9M projected (CBO) |
| House vote: | 218–214; Senate 51–50 (VP Vance tie-break) |
| HCBS risk: | States historically cut optional HCBS first when federal funding decreases |
| Work requirements: | 80 hours/month; exemption for medically frail (documentation required) |
| Key timeline: | Expansion FMAP sunsets Jan 2026; eligibility changes Oct 2026; work req Jan 2027 |
| ASAN (Zoe Gross): | States will cut HCBS first; disabled people lose lifeline services |
| ABA Medicaid growth: | 298% increase 2019–2024 (Trilliant Health) |
| State actions: | ID, MO, MD, CO, UT, WA considering HCBS reductions (Disability Scoop, Mar 2026) |
SOURCES & REFERENCES
| 1. | Disability Scoop. “Congress Approves Nearly $1 Trillion In Cuts To Medicaid.” July 3, 2025. |
| 2. | Disability Scoop. “Nation’s Disability Services System Faces Unprecedented Threats.” March 30, 2026. |
| 3. | Center for American Progress. “The Truth About the OBBBA’s Cuts to Medicaid and Medicare.” August 2025. |
| 4. | Urban Institute. “Medicaid Cuts in the OBBBA Leave 3 in 10 Young Adults Vulnerable.” August 2025. |
| 5. | American Psychological Association. “Update on Cuts to Medicaid Funding.” 2025. |
| 6. | Autism Society of America. “Autism Society Disheartened by Reconciliation Bill.” autismsociety.org. |
| 7. | U.S. News. “What’s Changing with Medicaid Eligibility.” health.usnews.com. |
| 8. | Clearbrook. “Impact of the OBBBA on Individuals with Disabilities.” August 2025. |