The Quiet Migration: What’s Moving Offshore
MEDELLÍN, COLOMBIA — The business process outsourcing industry in Colombia generated approximately $7 billion in revenue in 2022 and has been growing at 5 to 7 percent annually, according to the IT and Business Process Association of the Philippines’ global benchmarking data. The country’s BPO workforce exceeds 220,000 full-time equivalents. In the Philippines, the outsourcing sector is even larger — a foundational pillar of the national economy, employing over 1.5 million people and generating $33 billion in annual revenue. Healthcare-specific BPO is among the fastest-growing segments in both countries, with Latin American healthcare outsourcing projected to grow at roughly 10 percent annually through 2027.
ABA therapy companies have begun tapping into these markets. The functions being moved are overwhelmingly administrative, not clinical: insurance eligibility verification and benefits checks, prior authorization submission and follow-up, claims coding and submission using ABA-specific CPT codes, payment posting, accounts receivable management, denial management and appeals preparation, credentialing and payer enrollment, scheduling coordination, and data entry into practice management platforms like CentralReach, Rethink, and AlohaABA. These are tasks that require precision, healthcare literacy, and familiarity with U.S. payer systems — but do not require a BCBA credential, a clinical license, or physical proximity to the patient.
The companies making this move range from large PE-backed multi-state providers to mid-size regional practices, and they are doing so through a combination of direct offshore hiring, partnerships with healthcare-specialized BPO firms, and hybrid models that pair small domestic management teams with larger offshore execution teams. Few are discussing it publicly. The economics, however, are straightforward.
The Economics: What It Saves
A full-time medical biller or credentialing specialist in the United States earns $40,000 to $55,000 per year in salary, plus benefits that typically add 25 to 35 percent to total compensation. An equivalent role in Medellín or Manila costs $12,000 to $20,000 per year fully loaded — including salary, benefits, office space, technology, and management overhead charged by the BPO provider. The labor arbitrage is 50 to 70 percent, depending on the role and the market.
For an ABA practice billing $5 million per year with a five-person administrative team, the annual savings from offshoring those roles can exceed $150,000 — enough to fund a full-time BCBA position or absorb a Medicaid rate cut without reducing clinical staff. For larger organizations with 20 or 30 administrative employees, the savings scale into the hundreds of thousands, providing margin relief in an industry where reimbursement rates are stagnant or declining and prior authorization burdens are increasing.
The nearshore model — Colombia in particular — offers advantages beyond cost. Medellín and Bogotá operate in the Eastern and Central U.S. time zones, enabling real-time collaboration during business hours. Colombia’s workforce has strong English proficiency, particularly in the BPO sector, and cultural alignment with U.S. business practices. Direct flights from major U.S. cities take three to five hours, making site visits practical. The Philippines offers even deeper BPO infrastructure and a larger talent pool, but with a 12-to-13-hour time difference that typically requires overnight shifts for staff working on U.S. healthcare accounts.

Why ABA Is Particularly Suited — and Particularly Vulnerable
Several characteristics of the ABA industry make it an attractive candidate for administrative offshoring. The billing is session-based and time-driven, using a limited set of CPT codes (97151 through 97158, plus the Category III codes) that can be learned and applied by trained billing specialists regardless of geography. Prior authorization is required for virtually every patient and must be renewed every few months, creating a recurring administrative workload that is labor-intensive but procedurally consistent. Credentialing with multiple payers and managed care organizations is a months-long process that requires meticulous document management. And the industry’s chronic domestic staffing shortage means that administrative roles compete for the same limited labor pool as clinical positions.
At the same time, ABA’s reliance on offshoring introduces vulnerabilities that are specific to the field. ABA billing is not generic medical billing. The authorization process requires understanding of medical necessity criteria that vary by payer, state, and plan type. Denial management often requires clinical context — understanding why an authorization was reduced, what documentation is needed to appeal, and how to frame the clinical justification in language that Optum or BCBS or Medicaid will accept. An offshore billing team that lacks this clinical context may process claims efficiently but may not catch the nuances that determine whether a denial is worth appealing or how to prevent the next one.
HIPAA compliance is another consideration. Protected health information flows through every billing, scheduling, and credentialing transaction. Offshore teams must operate under the same HIPAA security standards as domestic teams, which requires business associate agreements, encrypted systems, access controls, workforce training, and audit capabilities. Reputable BPO providers in Colombia and the Philippines maintain SOC 2 Type II certification, HIPAA compliance programs, and physical security standards at their facilities. But the regulatory enforcement mechanisms are different: a HIPAA violation by a domestic employee triggers a well-understood enforcement pathway; a violation by an offshore contractor in a foreign jurisdiction introduces legal complexity that most ABA practice owners have never navigated.
What’s Not Moving: The Clinical Firewall
No ABA company of any size is offshoring clinical work. BCBA supervision, treatment plan development, direct therapy, parent training, and clinical decision-making remain entirely domestic — bound by state licensure requirements, payer credentialing rules, and the fundamental nature of the therapeutic relationship. The BACB’s certification requirements include supervised fieldwork that must be conducted in person or through approved telehealth modalities, and state behavior analyst licensure laws typically require that licensed practitioners be physically present in or licensed by the state where they deliver services.
But the line between administrative and clinical is not always clean. When an offshore scheduling coordinator decides which patients to prioritize for a BCBA’s caseload, that decision has clinical implications. When an offshore billing specialist reviews a denial and decides whether to appeal or accept it, that decision affects a child’s authorized hours. When an offshore credentialing team delays a payer enrollment, a BCBA cannot bill for services already delivered. The administrative layer is not separate from the clinical layer. It is the infrastructure on which clinical care depends.
Companies that offshore effectively recognize this interdependence and invest in integration: dedicated U.S.-based managers who oversee offshore teams, regular training on ABA-specific workflows, shared communication platforms that keep clinical and administrative teams in sync, and escalation protocols that ensure clinically consequential decisions are routed to domestic clinical staff. Companies that offshore poorly treat the administrative layer as a commodity, minimize the integration investment, and discover that cheap billing is expensive when it produces denials, delayed authorizations, and frustrated families.
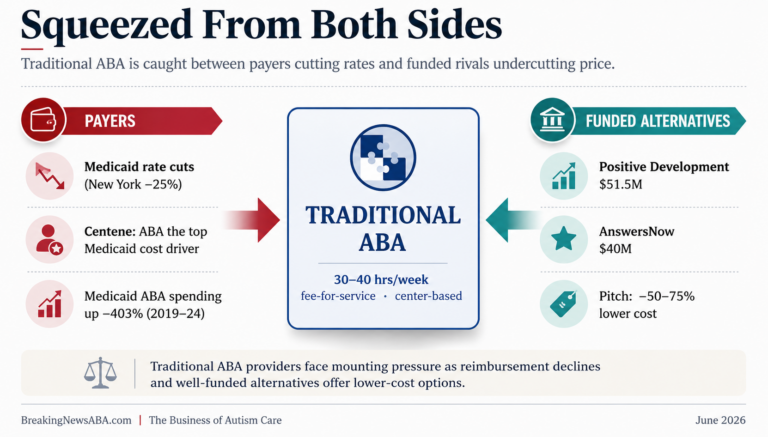
The Sustainability Question
The offshoring of ABA back-office operations is not a fad. It is a structural response to structural economics. Domestic administrative labor is expensive and scarce. ABA billing is complex and labor-intensive. Reimbursement rates are flat or declining. Prior authorization requirements are increasing. The margin pressure on ABA providers — particularly those serving Medicaid populations at rates well below the cost of care — is real and intensifying. Offshoring the administrative layer is one of the few levers available to reduce operating costs without cutting clinical staff or reducing patient hours.
The sustainability of the model depends on several factors. First, the quality of the offshore partner: healthcare-specialized BPO providers with experience in behavioral health billing will produce better outcomes than generalist outsourcing firms learning ABA on the job. Second, the investment in training and integration: offshore teams that are treated as an extension of the clinical operation, not a cost center, will perform closer to domestic standards. Third, the regulatory environment: if state licensing boards, payers, or CMS impose restrictions on the offshore handling of healthcare administrative data, the model could be constrained. Fourth, the competitive dynamics in the BPO markets themselves: as more U.S. healthcare companies nearshore to Colombia, wage inflation in Medellín and Bogotá will narrow the cost advantage, just as it has in other industries that concentrated in these cities.
For families, the offshoring of ABA administration is largely invisible. The parent who calls to check on an authorization status may not know whether the person tracking that authorization sits in Austin or Barranquilla. What they know is whether the authorization was obtained on time, whether their child’s hours were approved at the level the BCBA recommended, and whether the billing was handled correctly so they do not receive a surprise balance. The offshore model succeeds when families never have a reason to think about it. It fails when the distance between the person processing the claim and the child receiving the therapy produces errors, delays, or disconnects that families feel.
“The billing cycle begins when a child’s family requests service from a clinic. Before the appointment, the front-end staff checks whether the kid’s parents’ insurance covers an initial assessment.” — ABA billing workflow, Plutus Health
The ABA industry is following a path that hospitals, physician groups, and health systems have traveled for years: moving non-clinical operations to where the talent is most available and most affordable, while keeping clinical care local. The difference is that ABA is a younger, smaller, and more fragmented industry, with less institutional infrastructure for managing complex vendor relationships and less regulatory clarity about the boundaries of offshore healthcare administration. The companies that navigate this transition well will have a meaningful cost advantage. The companies that navigate it poorly will discover that the savings on billing staff are consumed by the cost of fixing the errors those staff produce.
AT A GLANCE
Trend: Growing number of U.S. ABA therapy companies offshoring administrative and back-office operations to Colombia (Medellín, Bogotá, Barranquilla) and the Philippines (Manila, Cebu)
Functions Offshored: Insurance eligibility/benefits verification; prior authorization submission and follow-up; claims coding and submission (CPT 97151–97158); payment posting; AR management; denial management; credentialing; scheduling; data entry
Functions NOT Offshored: BCBA supervision, treatment planning, direct therapy, parent training, clinical decision-making (bound by state licensure and BACB requirements)
Cost Savings: 50–70% labor arbitrage; U.S. biller: $40–$55K + benefits; offshore equivalent: $12–$20K fully loaded; potential $150K+ annual savings for a 5-person admin team
Colombia Advantages: U.S. time zone alignment (EST/CST); strong English proficiency; cultural compatibility; 3–5 hour direct flights; ranked #1 on Offshore BPO Confidence Index; $7B+ BPO industry; 220,000+ FTEs
Philippines Advantages: Largest BPO workforce globally (1.5M+ employees); $33B annual revenue; deep healthcare expertise; 12–13 hour time difference requires night shifts for U.S. accounts
Healthcare BPO Growth: Latin American healthcare BPO projected to reach $33B by 2027 at ~10% annual growth; 60%+ of U.S. healthcare providers plan to outsource RCM activities
HIPAA Considerations: Offshore teams must maintain BAAs, encrypted systems, access controls, workforce training; reputable providers hold SOC 2 Type II, HIPAA compliance programs
ABA-Specific Risks: ABA billing requires clinical context for denial management; authorization decisions have clinical implications; payer rules vary by state/plan; not generic medical billing
Integration Keys: U.S.-based managers overseeing offshore teams; ABA-specific training; shared communication platforms; escalation protocols for clinically consequential decisions
Practice Platforms: Offshore teams work within CentralReach, Rethink, AlohaABA, Theralytics, and other ABA practice management systems via cloud access
Industry Context: ABA admin offshoring driven by domestic labor scarcity, 65–104% turnover, stagnant reimbursement rates, increasing PA burdens, and margin pressure on Medicaid populations
Sustainability Risks: Wage inflation in nearshore markets; regulatory changes; quality variance among BPO providers; clinical-administrative interdependence; vendor management complexity
Family Impact: Ideally invisible to families; success = timely authorizations, correct billing, no surprise balances; failure = delays, errors, disrupted care
SOURCES & REFERENCES
Colombia BPO Data: IT and Business Process Association of the Philippines (IBPAP) global benchmarking; NeoWork healthcare RCM outsourcing analysis (November 2025); Auxis healthcare BPO market report
Philippines BPO Data: IBPAP; Unity Communications Philippine outsourcing industry statistics (April 2025); NeoWork medical billing outsourcing analysis (September 2025)
Healthcare BPO Trends: Market Data Forecast (2023); RevCycleIntelligence provider outsourcing survey; Medical Device News nearshore outsourcing report; Grey Matter Innovationz healthcare BPO analysis (October 2025)
ABA Billing Complexity: Plutus Health ABA billing guide; ABA Coding Coalition CPT code resources; Cube Therapy Billing industry analysis; AnnexMed ABA billing company review (2025)
ABA Workforce Data: CentralReach 2025 Autism and IDD Care Market Report (turnover rates); BHCOE median turnover data; BACB certificant and demand data (2025)
HIPAA & Compliance: HHS HIPAA Security Rule; SOC 2 Type II certification standards; BAA requirements for offshore contractors under 45 CFR §164.502(e)
Nearshore Providers: Auxis (Costa Rica/Colombia); Vinali Group (Colombia); SuperStaff (Medellín); NeoWork; Connect2BPO; Nearbridge Global
Published: BreakingNewsABA.com — March 2026