Why ABA Billing Is Different
ACROSS THE UNITED STATES – a single ABA client session can generate a billing record that no other outpatient specialty in healthcare routinely produces. A child receiving four hours of direct ABA therapy in a clinic may produce a claim that includes 16 units of CPT code 97153 for direct treatment delivery by a registered behavior technician, two units of 97155 for BCBA protocol modification and supervision conducted during the session, and one unit of 97156 for caregiver training delivered at pickup. Each code is time-based, billed in 15-minute increments, and subject to modifier requirements that specify the rendering provider’s credential level, the place of service, and whether the session was delivered individually or in a group setting.
The complexity compounds at the authorization layer. Most commercial insurers and Medicaid managed care plans require prior authorization for ABA services, typically renewed every six months. The authorization specifies the number of approved hours per week, the approved CPT codes, the authorized date range, and in many cases the specific rendering providers. A single authorization error — a session that exceeds the approved hours, a provider whose credential has not been linked to the authorization, a code billed outside the authorized date range — produces a denial that requires manual rework.
The result is a billing environment that differs from most medical specialties in three structural ways. First, the volume of line items per patient is exceptionally high. A child receiving 25 hours per week of ABA therapy generates roughly 100 units of billable service per week, or more than 5,000 units per year — compared to a psychotherapy patient who generates one unit per weekly session. Second, the authorization management burden is continuous rather than episodic; ABA providers must track authorization utilization in real time to avoid both under-utilization (which can lead to reduced future authorizations) and over-utilization (which produces denials). Third, the payer landscape is fragmented: a single ABA practice may bill Medicaid fee-for-service, multiple Medicaid managed care plans, and several commercial insurers, each with its own authorization protocols, fee schedules, modifier rules, and claim submission formats.
A single ABA client receiving 25 hours of weekly therapy generates more than 5,000 billable units per year. No other outpatient behavioral health specialty produces claim volumes at this scale per patient, and no other specialty requires the same density of real-time authorization tracking.
Industry data consistently identifies ABA claim denial rates in the range of 15 to 25 percent for practices without dedicated billing infrastructure — materially higher than the healthcare industry average of approximately 5 to 10 percent reported by the American Medical Association. The most common denial reasons are authorization-related: services rendered outside the authorized date range, units exceeding the authorized quantity, and credentialing mismatches between the rendering provider and the payer’s records. Each denied claim represents revenue that must be appealed, rebilled, or written off — and the cost of reworking a denied ABA claim can exceed the cost of processing it correctly the first time.
The ABA CPT Code Architecture
The current CPT code set for ABA therapy was established by the American Medical Association in 2019, replacing a patchwork of Category III temporary codes that the industry had operated under since 2014. The permanent Category I codes — 97151 through 97158 — formalized the distinction between assessment, direct treatment, supervision, and caregiver training, and established the 15-minute unit structure that now governs ABA billing nationwide.
97151 — Behavior identification assessment: the initial and reassessment evaluation conducted by a qualified healthcare professional (BCBA or equivalent). Billed in 15-minute units, typically authorized for the initial evaluation and periodic reassessments.
97152 — Behavior identification-supporting assessment: administered by a technician under BCBA direction. Used for structured data collection that supports the formal assessment.
97153 — Adaptive behavior treatment by protocol: the workhorse code of ABA billing. This is the direct, one-on-one treatment delivered by an RBT or behavior technician following a BCBA-designed protocol. For most ABA practices, 97153 represents 70 to 85 percent of total billed units.
97155 — Adaptive behavior treatment with protocol modification: BCBA-delivered treatment that includes real-time clinical decision-making and protocol adjustment. This code captures the supervisory and clinical oversight layer that distinguishes ABA from technician-only delivery models.
97156 — Family adaptive behavior treatment guidance: BCBA-delivered caregiver training. Increasingly emphasized by payers as a required component of treatment plans, particularly for early-intervention populations.
The billing complexity emerges not from the codes themselves but from their interaction with payer-specific rules. Some commercial insurers require modifier 95 for synchronous telehealth delivery of 97155 and 97156; others use modifier GT or place-of-service code 02. Some Medicaid plans allow concurrent billing of 97153 and 97155 when the BCBA provides supervision during a technician-delivered session; others require the codes to be billed on separate service lines with non-overlapping time stamps. Some payers apply a per-day unit cap on 97153; others cap by authorization period. The permutations generate a compliance matrix that grows with every payer contract a practice signs.
The RCM Ecosystem: Who the Players Are
The ABA revenue cycle management market has stratified into three tiers, each serving a distinct segment of the provider landscape.
Tier 1 — Integrated platform companies: CentralReach, the dominant ABA practice management platform, offers end-to-end RCM services layered on top of its clinical data collection, scheduling, and billing software. Backed by Insight Partners, CentralReach has pursued an acquisition strategy that has expanded its capabilities across the ABA operational stack, including the 2021 acquisition of WebABA, a competing practice management system. The integration of RCM with the clinical platform creates a data advantage: because the billing team operates within the same system where clinicians document sessions and track authorizations, the claim scrubbing process can flag errors before submission rather than after denial.
Therapy Brands, backed by KKR, operates a parallel model through its Catalyst platform (formerly known as Catalyst by Therapy Brands). Catalyst combines practice management, clinical documentation, and billing into a single ABA-specific platform, with optional RCM services that handle claim submission, denial management, and payment posting. The Therapy Brands portfolio also includes platforms serving adjacent behavioral health specialties, creating cross-selling opportunities as ABA practices diversify into speech, occupational therapy, and mental health services.
Tier 2 — Specialized ABA billing companies: a mid-market layer of companies that provide outsourced billing and RCM services specifically for ABA practices without building their own practice management software. These firms employ billing specialists who are trained in ABA-specific CPT codes, modifier rules, and authorization management workflows. They typically integrate with whatever practice management platform the provider already uses — CentralReach, Catalyst, or smaller systems — and handle the downstream revenue cycle from claim creation through payment posting and denial resolution.
The specialized ABA billing company model has grown because it addresses a specific operational reality: most ABA practices are founded by BCBAs whose training is clinical, not financial. A BCBA who opens a practice with five RBTs and 30 clients may be an excellent clinician but has no background in CPT coding, payer contracting, or denial management. The specialized billing company provides that capability on a variable-cost basis, typically charging between 5 and 8 percent of collected revenue or a per-claim fee that ranges from $4 to $8 depending on claim volume and complexity.
Tier 3 — General healthcare RCM with ABA divisions: national revenue cycle management companies that have added ABA-specific teams as the specialty’s billing volume has grown large enough to justify dedicated capacity. These firms bring scale advantages in clearinghouse relationships, payer connectivity, and denial analytics but may lack the deep ABA-specific expertise of Tier 1 and Tier 2 providers. Their value proposition is typically strongest for large, multi-state ABA organizations that need a single RCM vendor capable of handling commercial, Medicaid, and managed care billing across diverse payer environments.
The typical ABA RCM engagement charges between 5 and 8 percent of collected revenue. For a mid-size practice collecting $3 million annually, that represents $150,000 to $240,000 in RCM fees — the cost of approximately two full-time billing staff, but with the infrastructure, payer expertise, and denial management capacity that two employees cannot replicate.
The Authorization Management Problem
Authorization management has emerged as the single most operationally intensive component of ABA revenue cycle management, and the capability that most directly drives outsourcing decisions. The authorization lifecycle in ABA is not a one-time event; it is a continuous process that begins with the initial authorization request, requires real-time utilization tracking throughout the authorized period, demands proactive re-authorization submissions before the current authorization expires, and generates immediate revenue consequences when any step fails.
A typical ABA client on a 25-hour-per-week treatment plan requires a new authorization or re-authorization every 90 to 180 days, depending on the payer. Each re-authorization submission includes updated clinical documentation — progress reports, treatment plan revisions, assessment data — that must demonstrate medical necessity and measurable progress toward treatment goals. Payers have become increasingly rigorous in their re-authorization review criteria, and denial of re-authorization requests has become a material revenue risk for ABA practices.
The operational math is straightforward. A practice with 100 active clients, each requiring re-authorization two to four times per year, must manage 200 to 400 authorization cycles annually. Each cycle involves preparing clinical documentation, submitting the request through the payer’s portal or fax system, tracking the response timeline, responding to requests for additional information, and logging the approved parameters. A single missed re-authorization deadline means a gap in coverage that can suspend services for a client and eliminate revenue for the practice until the authorization is reinstated.
Several ABA-specific software tools have emerged to address authorization tracking, including features built into CentralReach and Catalyst that generate automated alerts when authorizations approach expiration or utilization thresholds. Third-party authorization management tools that integrate with practice management platforms have also entered the market, offering dashboard visibility into authorization status across the entire client population. But the underlying problem remains structural: ABA’s authorization burden is a function of payer policy, and no amount of software sophistication eliminates the clinical documentation work required to satisfy re-authorization criteria.
Why the Outsourcing Trend Is Accelerating
Three forces are driving an increasing share of ABA practices toward outsourced revenue cycle management.
The talent gap in ABA billing: the pool of billers and coders with ABA-specific expertise is small relative to demand. General medical billers can be retrained on ABA CPT codes, but the modifier rules, authorization workflows, and payer-specific requirements create a learning curve that takes six to twelve months to navigate competently. Turnover in billing staff — which industry surveys consistently place above 20 percent annually in healthcare — means practices that maintain in-house billing teams face recurring recruitment and training costs. Outsourced RCM providers amortize that expertise across their client base, making the cost of a specialized biller fractional rather than fixed.
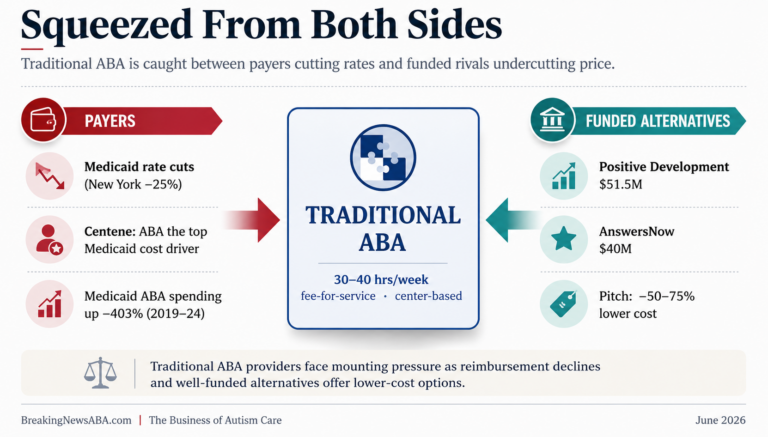
Margin pressure from rate compression: Medicaid reimbursement rates for ABA have been flat or declining in real terms across most states, and commercial payers have used their market leverage to push contracted rates downward as the ABA provider supply has expanded. When rates compress, revenue cycle efficiency becomes a margin lever rather than an administrative function. A practice that reduces its denial rate from 20 percent to 8 percent and shortens its average days in accounts receivable from 60 to 35 recovers working capital that directly impacts profitability. Outsourced RCM providers market exactly this value proposition: not cost savings on billing staff, but revenue recovery from claims that would otherwise be denied, delayed, or written off.
PE-driven professionalization: private equity firms that have acquired ABA practices have uniformly moved to standardize and professionalize revenue cycle operations across their portfolios. For a PE-backed platform operating 20 or 50 clinic locations across multiple states, the in-house billing model that worked for a single-location founder-led practice does not scale. Platform operators have driven significant volume toward the Tier 1 integrated platforms, both because the PE playbook prioritizes operational standardization and because the data visibility that integrated platforms provide — real-time dashboards showing collections, denial rates, days in AR, and authorization utilization by clinic — aligns with the financial reporting cadence that PE investors require.
Market Size and the Economics of ABA RCM
Estimating the total addressable market for ABA revenue cycle management requires working from the industry’s aggregate billing volume. The ABA therapy industry generated an estimated $8 billion to $10 billion in total U.S. revenue in 2024, combining Medicaid, commercial insurance, and self-pay sources. If RCM costs represent approximately 8 to 12 percent of collected revenue when accounting for both direct billing fees and the internal labor cost of revenue cycle activities, the total spend on ABA revenue cycle management — inclusive of outsourced services, in-house billing staff, practice management software, clearinghouse fees, and credentialing services — falls in the range of approximately $800 million to $1.2 billion.
The outsourced segment of that market is smaller but growing faster. Industry observers estimate that between 40 and 50 percent of ABA practices now outsource some or all of their revenue cycle management, up from an estimated 25 to 30 percent five years ago. Applying the outsourced share to the total RCM spend suggests a directly addressable outsourced RCM market in the range of $400 million to $600 million, with the remainder locked in internal billing operations that represent a conversion opportunity for RCM vendors.
The unit economics for outsourced ABA RCM providers are attractive. The percentage-of-collections model aligns the vendor’s revenue with the practice’s revenue, creating a built-in growth mechanism as practices add clients. The labor model is scalable: ABA billing specialists can manage portfolios of 60 to 100 clients per full-time equivalent, and the work is largely systematizable, with rules-based claim scrubbing, templated authorization submissions, and standardized denial appeal workflows. The result is gross margins that industry participants describe as being in the range of 40 to 55 percent for established RCM operations with sufficient scale.
The market has not yet produced a public company or a large-scale exit that would provide definitive financial data. But the PE interest in the adjacent practice management layer — Insight Partners’ investment in CentralReach, KKR’s ownership of Therapy Brands — suggests that sophisticated financial sponsors view the ABA operational infrastructure as a durable, high-margin business tied to a structural demand curve.
What This Means for ABA Practice Owners
For ABA practice owners evaluating their revenue cycle strategy, the decision framework has shifted. Five years ago, the question was whether to outsource billing. Today, the question is what to outsource and to whom.
Small practices — single-location operations with fewer than 50 clients — face the starkest build-versus-buy calculation. An in-house biller costs between $45,000 and $65,000 in annual salary plus benefits, training, software licenses, and management overhead. That biller represents a single point of failure: if they leave, the practice’s revenue cycle stops until a replacement is trained. An outsourced RCM provider at 6 percent of collections on a $1.5 million practice costs approximately $90,000 per year — more than a single in-house biller, but with redundancy, payer expertise across multiple plans, and denial management infrastructure that a single employee cannot match.
Mid-size practices — multi-location operations collecting between $3 million and $15 million — have more options but face a different risk. At this scale, the practice can justify a small internal billing team, but the authorization management burden and payer complexity often exceed what a two-to-three-person team can handle without errors. The hybrid model, where the practice maintains internal authorization and clinical documentation staff while outsourcing claim submission and denial management, has gained traction in this segment.
Large platform operators — PE-backed organizations with 20 or more locations — are increasingly building internal revenue cycle operations on top of integrated platform technology, bringing the function in-house at a scale where the unit economics favor it. At this tier, the practice is not buying RCM services; it is building an RCM capability that becomes a competitive advantage and, in some cases, an infrastructure asset that could eventually be offered as a service to smaller practices in its network.
The market for ABA revenue cycle management exists because ABA billing is structurally harder than what most healthcare specialties require. That complexity is not going away. The CPT code structure, the authorization burden, and the payer fragmentation are embedded in the operational reality of delivering ABA therapy. For as long as those conditions persist, the back-office industry built to manage them will continue to grow alongside the clinical industry it supports.
AT A GLANCE
ABA industry revenue (est. 2024): Approximately $8–10 billion in total U.S. revenue across Medicaid, commercial, and self-pay sources
ABA RCM total spend (est.): Approximately $800 million–$1.2 billion including in-house and outsourced billing operations
Outsourcing rate: An estimated 40–50% of ABA practices now outsource some or all RCM, up from approximately 25–30% five years ago
Typical RCM fee structure: 5–8% of collected revenue (percentage model) or $4–$8 per claim (per-claim model)
Key CPT codes: 97151–97158 (Category I, established 2019); 97153 represents 70–85% of billed units at most practices
ABA denial rates: 15–25% for practices without dedicated billing infrastructure vs. 5–10% healthcare average (AMA)
Authorization cycle: Re-authorization required every 90–180 days per client per payer, with clinical documentation
CentralReach: Dominant ABA platform; backed by Insight Partners; acquired WebABA (2021)
Therapy Brands / Catalyst: ABA practice management and RCM platform; backed by KKR
In-house biller cost: $45,000–$65,000 annual salary plus benefits, training, and software; single point of failure at small practices
PE impact: Platform operators standardizing RCM across multi-state portfolios, driving Tier 1 platform adoption
SOURCES & REFERENCES
1. – American Medical Association. CPT Codes 97151–97158: Adaptive Behavior Services. CPT Code Set. Effective January 2019.
2. – American Medical Association. Claim Denial Benchmark Data. National Health Insurer Report Card. Published annually.
3. – CentralReach. Platform and RCM Services Overview. centralreach.com.
4. – Therapy Brands. Catalyst Practice Management Platform. therapybrands.com.
5. – Insight Partners. CentralReach Investment Announcement. Press release. 2021.
6. – KKR. Therapy Brands Acquisition Announcement. Press release.
7. – Council of Autism Service Providers (CASP). ABA Practice Operations Survey Data. Published periodically.
8. – Behavioral Health Business. ABA Industry Revenue and Market Size Analysis. Multiple reports, 2023–2025.
9. – Centers for Medicare & Medicaid Services (CMS). Medicaid Behavioral Health Services Expenditure Data. medicaid.gov.
10. – BACB (Behavior Analyst Certification Board). Certificant Data and Workforce Statistics. bacb.com. Updated annually.