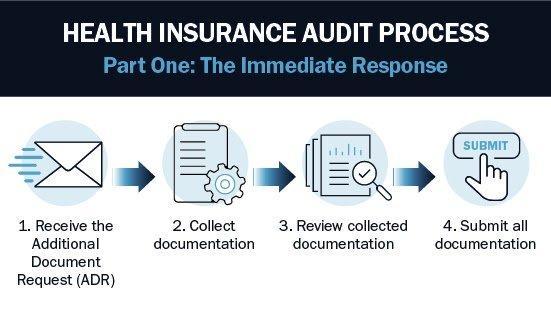
ATLANTA — The letter arrives without warning. A Blue Cross Blue Shield affiliate requests medical records for a sample of patients and dates of service — typically 20 to 30 claims selected from the provider’s billing history over a one- to three-year period. The provider has 30 to 45 days to produce the documentation. A clinical review team compares the records against the plan’s billing policies and procedures — many of which are not in the provider contract but are buried in the payer’s reimbursement manual. If the reviewers find errors, the plan calculates a deficiency rate from the sample, extrapolates that rate across the provider’s entire universe of BCBS-financed patients for the applicable period, and issues a recoupment demand.
The demand can be enormous. A provider with $2 million in annual BCBS revenue and a 15% deficiency rate on the sample faces a potential recoupment of $300,000 per year under review — and audits frequently cover two or three years. Healthcare attorneys who represent ABA practices report that recoupment demands in the six figures are routine and that demands exceeding $500,000 are not uncommon. Some practices have faced demands that threatened their solvency.
This is not a story about fraud. The providers receiving these audit letters are, in most cases, delivering clinically appropriate ABA therapy to autistic children whose treatment was pre-authorized by the same BCBS plan now demanding money back. The gap is between the clinical work being done and the documentation trail the payer requires — and the consequences of that gap, amplified by statistical extrapolation, are reshaping the financial landscape of the ABA industry.
33 Companies, 33 Sets of Rules
Blue Cross Blue Shield is not a single insurer. It is a federation of 33 independent, locally operated health insurance companies. Each affiliate — Anthem, Highmark, Florida Blue, BCBS of Illinois, BCBS of Alabama, BCBS of Massachusetts, and the rest — sets its own fee schedules, billing rules, documentation requirements, and audit protocols. A provider operating in three states may be subject to three entirely different sets of rules governing the same CPT codes for the same service. What constitutes compliant documentation in one state may be deficient in another.
This fragmentation is the first structural problem. ABA providers, particularly multi-state organizations backed by private equity, have scaled rapidly across state lines. Their billing and documentation systems are often standardized internally — but BCBS affiliates are not standardized with each other. A session note template that passes audit in Massachusetts may lack a required element in Georgia. A supervision log format that satisfies Anthem may be insufficient for Highmark. The provider discovers the discrepancy only when the audit letter arrives.
Anthem’s ABA Provider Resource Guide, published in June 2025 and spanning multiple states including Connecticut, Georgia, Indiana, Kentucky, and Virginia, illustrates the specificity of the requirements: session notes must include the six- or eight-digit date, start and end times for every timed and untimed code, the rendering provider’s credentials, and documentation that directly ties each billed unit to clinical activity performed. NCCI edits and Medically Unlikely Edits are applied to flag billing patterns that exceed statistical norms. Providers whose claim patterns “vary significantly from peers” may face not only audits but reinstatement of prior authorization requirements that had previously been waived.
![In many ABA programs, 60 to 80 percent of denial root causes trace to documentation problems rather than billing errors — shifting documentation from a clinical admin task to a core revenue cycle control point. | Photo courtesy: [attribution]](https://breakingnewsaba.com/wp-content/uploads/2026/04/bcbs-article-image-2-3.jpg)
What Triggers an Audit — and What Auditors Look For
BCBS affiliates use claims data analytics to identify providers whose billing patterns deviate from statistical norms. The triggers are algorithmic, not personal. Common flags include: high total units billed per patient per month, particularly on CPT code 97153 (adaptive behavior treatment by protocol, the code that accounts for the vast majority of RBT-delivered therapy hours); billing for services by non-credentialed providers; overlapping service times across patients; and patterns of billing at the maximum units allowed without variation.
Once the audit is initiated, reviewers evaluate the selected claims against a checklist that is payer-specific and often more granular than providers expect. The most common deficiency categories reported by healthcare attorneys and billing consultants working with ABA practices include: missing or incomplete parent/guardian signatures on treatment plans and initial assessments; session notes that lack specificity or fail to demonstrate medical necessity for each billed unit; notes that do not clearly link the intervention performed to the treatment plan goals; incorrect or missing provider credentials; inaccurate time tracking, including start/end times that do not match billed units; and documentation that fails to articulate why the service was needed at that intensity on that date.
The clinical quality of the therapy is not what the audit measures. The audit measures whether the documentation trail, as recorded, satisfies the payer’s administrative requirements at the moment of review. A provider can deliver exceptional clinical care, produce measurable patient outcomes, and still fail an audit because the session note said “worked on communication” instead of specifying which communication skill was targeted, what prompts were used, and how the patient responded across measured opportunities.
![ABA therapy is among the most documentation-intensive services in behavioral health: high-frequency sessions, multiple provider types (BCBA, RBT, BCaBA), time-based billing codes, and payer-specific rules that differ across every BCBS affiliate. | Photo courtesy: [attribution]](https://breakingnewsaba.com/wp-content/uploads/2026/04/bcbs-article-image-3-3.jpg)
The BCBSIL Modifier Shift: A Case Study in Moving Targets
Blue Cross Blue Shield of Illinois provides an instructive example of how BCBS affiliates are reshaping ABA reimbursement through administrative policy changes that function as de facto rate adjustments — and create new audit exposure for providers who fail to adapt quickly enough.
Effective January 1, 2024, BCBSIL implemented tiered payment rates for CPT code 97153, the primary code for direct ABA therapy. Providers must now append a modifier to every 97153 claim indicating the credential level of the rendering clinician. Modifier HN (RBT, BCaBA, or bachelor’s-level clinician) pays the baseline rate. Modifier HO (BCBA, BCBA-D, or master’s-level clinician) pays 20% above baseline. Modifier HM (clinician with less than a bachelor’s degree and no RBT certification) pays 20% below baseline. If no modifier is included, the claim defaults to the HM rate — the lowest tier.
The policy creates a documentation trap. A provider whose billing system does not automatically append the correct modifier to every 97153 claim will be underpaid on every session delivered by an RBT or BCBA — and correcting the underpayment retroactively requires resubmission of every affected claim. For a practice billing 10,000 units of 97153 per month, the administrative burden is substantial. And for providers who fail to include any modifier, the default to the lowest rate represents a 20% effective pay cut that many did not anticipate.
What Providers Can Do — Before the Letter Arrives
The providers who survive BCBS audits with minimal financial damage share a common profile: they treat documentation as a revenue cycle function, not a clinical afterthought. The following practices, drawn from healthcare attorneys, billing consultants, and compliance specialists who work with ABA organizations, represent the current best-practice framework for audit readiness.
Conduct internal audits before the payer does. Review a random sample of charts quarterly, using each payer’s specific documentation requirements as the audit checklist. The goal is to identify template deficiencies, training gaps, and documentation patterns that would fail an external review — and fix them before the payer finds them. In many ABA programs, 60 to 80 percent of denial root causes trace to documentation problems rather than billing errors.
Know each payer’s specific rules — not just the CPT codes. BCBS affiliates publish their requirements in provider manuals, medical policies, clinical payment and coding policies, and resource guides. These documents are not identical across affiliates. A practice operating under Anthem in Virginia and BCBS of Illinois must maintain two separate compliance frameworks. Read the manuals. Update your templates when the manuals change.
Credential every BCBA individually. Most major payers, including BCBS, require individual credentialing for each BCBA providing billable services. Billing under another provider’s credentials while “waiting” for credentialing is a red flag that can trigger recoupment of all paid claims for services rendered by the non-credentialed provider — sometimes going back years.
Build session note templates that are payer-specific and audit-proof. Every note should connect the service provided to the diagnosis and treatment plan goals. Specify which skill was targeted, what intervention was used, what prompts were delivered, and how the patient responded with measurable data. Avoid vague language. “Worked on communication” is an audit red flag. “Targeted requesting preferred items using PECS card independently across 5 opportunities; 3/5 independent, 2/5 with gestural prompt” is defensible.
Respond to audit requests with legal counsel. The 30- to 45-day window to produce records is a legal proceeding, not a routine administrative request. The provider’s response shapes the audit outcome and the recoupment calculation. Healthcare attorneys who specialize in payer audits can identify sampling defects, challenge extrapolation methodology, negotiate reduced repayment amounts, and ensure the provider exhausts all internal appeal rights before any payment is returned.
![The practices that survive BCBS audits with minimal financial damage share a common profile: they treat documentation as a revenue cycle function, not a clinical afterthought — and they conduct internal audits on a quarterly cycle before the payer does. | Photo courtesy: [attribution]](https://breakingnewsaba.com/wp-content/uploads/2026/04/bcbs-article-image-4-3.jpg)
The Bigger Picture: Audits as Rate Reduction by Other Means
The intensification of BCBS audit activity against ABA providers is not happening in isolation. It is part of a broader payer strategy to manage the cost of a benefit category that has grown faster than almost any other in commercial insurance. ABA therapy is high-frequency, high-intensity, and high-cost. A child receiving 30 hours per week of direct therapy at $60 to $80 per unit generates annual claims of $90,000 to $125,000 or more. Multiply that across a growing patient population and the payer’s financial incentive to reduce payouts becomes obvious.
Rate cuts are visible and generate political opposition from families and providers. Audits and retroactive recoupments achieve a similar financial result with less visibility. The provider receives a demand, pays or negotiates, and the transaction is governed by the confidentiality provisions of the provider agreement. There is no public hearing, no legislative session, no protest at the state capitol. The money simply moves from the provider’s account back to the payer.
This does not mean the audits are illegitimate. Documentation requirements exist for valid reasons — to verify that services were rendered as billed, to ensure medical necessity, and to protect patients from billing for services never provided. The federal and state audits that identified tens of millions of dollars in improper Medicaid ABA payments in Indiana, Wisconsin, and Minnesota demonstrate that fraud and overbilling are real problems in the ABA industry. But the application of extrapolation to documentation technicalities — where the clinical service was delivered, the patient benefited, and the only deficiency is an administrative omission — raises questions about whether the audit program is functioning as quality assurance or as a revenue recovery operation.
For providers, the practical distinction doesn’t matter. The recoupment demand arrives regardless of intent. The only defense is preparation — and the ABA practices that are investing in documentation quality, internal audit programs, payer-specific compliance training, and legal counsel for audit response are the ones that will remain standing when the next letter arrives.
AT A GLANCE
| BCBS Structure: | Federation of 33 independent affiliates; each sets its own billing rules, documentation requirements, and audit protocols |
| Audit Trigger: | Claims data analytics flagging billing patterns that deviate from statistical norms — high units/month, non-credentialed providers, overlapping times |
| Sample Size: | Typically 20–30 claims selected over 1–3 year review period |
| Extrapolation: | Deficiency rate from sample applied to provider’s entire BCBS-financed claims volume for audit period |
| Common Deficiencies: | Missing signatures; vague session notes; no link to treatment goals; incorrect credentials; time-tracking gaps |
| Recoupment Scale: | Six-figure demands routine; $500K+ not uncommon; multi-year lookback periods |
| BCBSIL Modifier: | Tiered rates for 97153 effective Jan 2024 — HN (baseline), HO (+20%), HM (−20%); no modifier defaults to lowest tier |
| Root Cause: | 60–80% of denial/recoupment root causes trace to documentation problems, not billing errors |
| Best Defense: | Quarterly internal audits; payer-specific templates; individual BCBA credentialing; legal counsel for audit response |
| State Protections: | Vary widely; some states limit recoupment timeframes (6 months to several years); check state insurance laws |
Sources & References
1. Anthem Blue Cross and Blue Shield. ABA Provider Resource Guide. June 2025
2. BCBS of Illinois. “Implementation of Tiered Rate Modifiers for ABA.” September 2023 / January 2024
3. BCBS of Illinois / Oklahoma. “Reduced Prior Authorization Requirements for Certain ABA Codes.” September 2022
4. ABA Building Blocks. “Clinical Documentation Compliance.” December 2024
5. ABA Building Blocks. “BCBA Credentialing & Billing Newsletter.” April 2025
6. Little Health Law. “Preparing Your ABA Company for a Payor Audit.” August 2024
7. Jackson LLP. “Insurance Clawbacks in Healthcare: What You Need to Know.” 2022
8. Revenue Cycle Blog. “ABA Documentation Audits: How to Protect Revenue in 2025.” December 2025
9. Brellium. “Prevent ABA Insurance Clawbacks with AI Session Audits.” 2025
10. Cube Therapy Billing. “ABA Billing Services: The 2025–2026 Playbook.” March 2026
11. MedStates. “ABA Therapy Billing Services: Nationwide RCM Support.” October 2025
12. PROMBS. “Blue Cross Blue Shield Therapy Reimbursement Guide 2025.” December 2025
13. Praxis Notes. “Medicaid ABA Documentation Cuts 2025: Compliance Guide.” January 2026
14. BCBS of Massachusetts. “Applied Behavior Analysis (ABA) Medical Policy.” June 2025