A handoff problem nobody is solving
INDIANAPOLIS. Ten years inside applied behavior analysis clinics taught Gracyn Conner that the hardest part of a hygiene routine is not the routine. It is the handoff. A client masters toothbrushing or hair brushing or nail filing in clinic. A registered behavior technician resigns. A new RBT starts cold. The family carries a paper sheet home that nobody can quite execute. Within weeks the skill regresses, the meltdowns return, and the BCBA is back at the start of a task analysis the client had already completed once.
That pattern is the origin of Hygiene Hippie. Conner is a pediatric occupational therapist with a decade of practice in and around ABA settings, an Assistant Professor and Academic Fieldwork Coordinator in the Department of Occupational Therapy at Marian University in Indianapolis, and the founder of a mobile app she built specifically for the moment a routine has to survive a staff change.
Conner holds an OTD and an MS and is a registered occupational therapist (OTR). Her academic affiliation is verified through the Marian University faculty directory. The product, Hygiene Hippie, is currently in pilots with ABA clinics, residential providers, vocational programs, and family caregivers across Indiana, with a national rollout planned. The thesis is narrow and operational: the science behind ABA hygiene work is solid, the access to that science in a portable format is not, and the gap shows up every time a staff member quits.
Conner does not market Hygiene Hippie as a clinical platform or a billing tool. She markets it as the layer that holds the routine together when the people delivering it change. Whether that framing carries through to outcome data is the test the next twelve to twenty-four months of pilots will start to answer.
Why ABA tech missed the front line
Most ABA software was built for the BCBA, the operations manager, and the biller. Practice management platforms route schedules and authorizations. Data collection systems capture trial-by-trial responses. Electronic medical records hold treatment plans and progress notes. The category leaders in operator software are designed around the clinician’s administrative day and the company’s revenue cycle. They are not designed around the moment a routine actually has to be delivered, by whoever is on shift, in whatever bathroom or kitchen or community setting the client happens to be in.
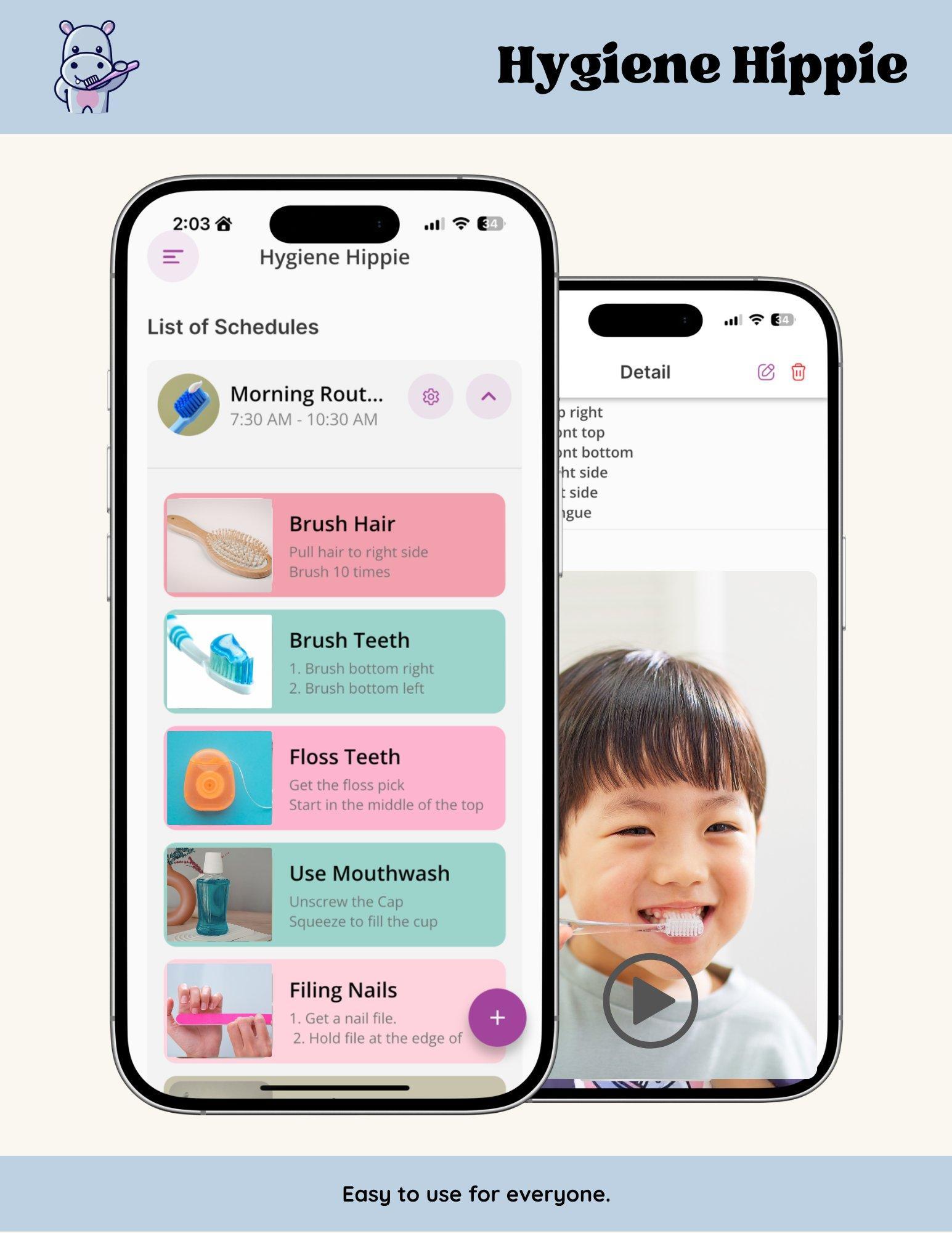
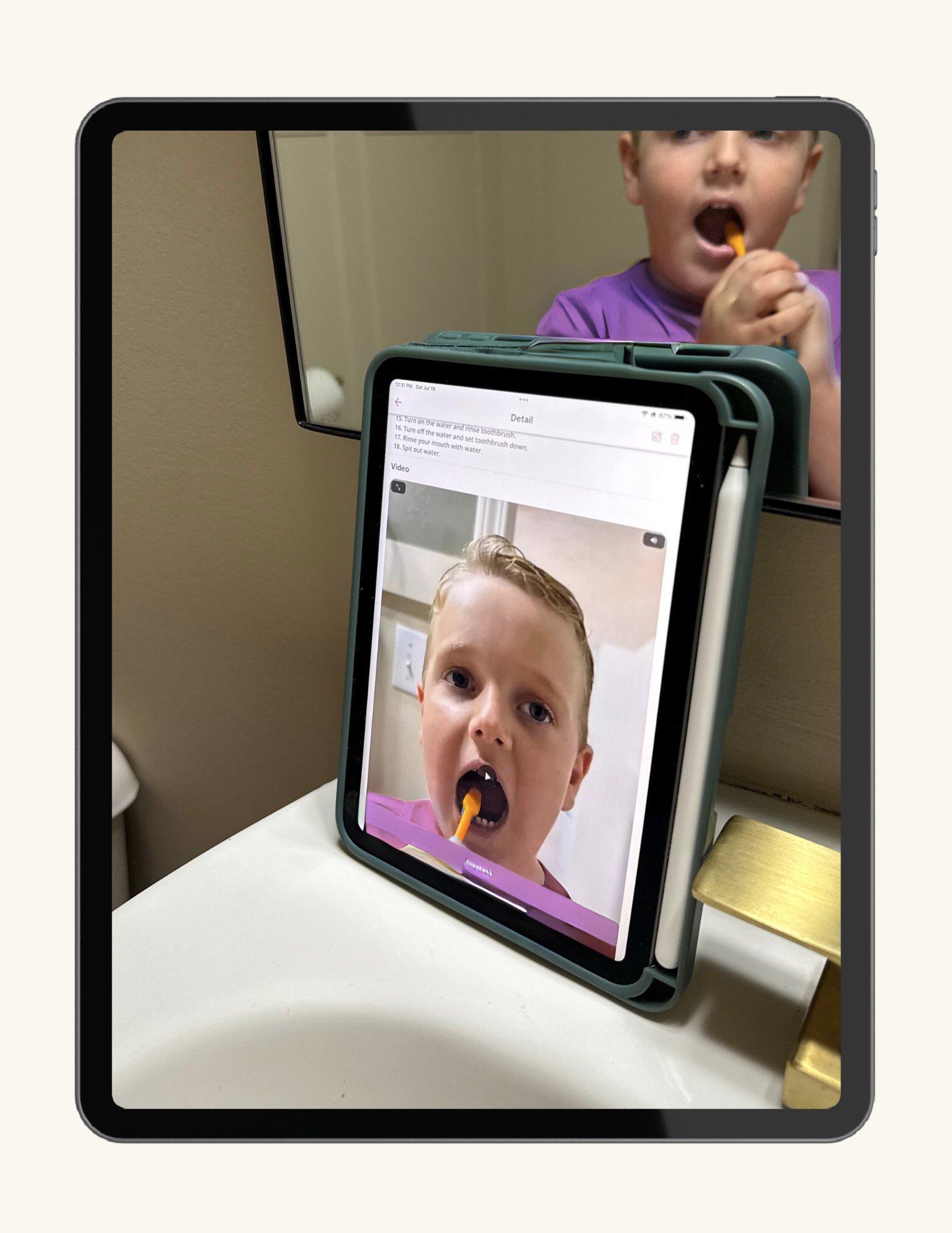
That delivery moment is where Hygiene Hippie sits. Per the company’s own materials, the app collects no protected health information, requires no client account, stores routines on the user’s own device, and can be passed from a clinic team to a family by sharing a code. A morning hygiene plan built once by an OT or a BCBA can be opened on the client’s tablet at home, on the parent’s phone in a hotel room on vacation, or on whatever device the next RBT happens to carry into the session.
The competitive frame here is not against the practice-management incumbents. It is against the absence of any product at the delivery layer at all. For most clients, that layer is currently a laminated picture schedule, a verbal rundown from the outgoing RBT, and a parent guess. Conner’s argument is that a layer that simple, that important, and that often broken is worth its own software category.
“Your team and your families deserve better tools than a handwritten sheet and a verbal rundown. This is mine.” Gracyn Conner, Founder, Hygiene Hippie (2025)
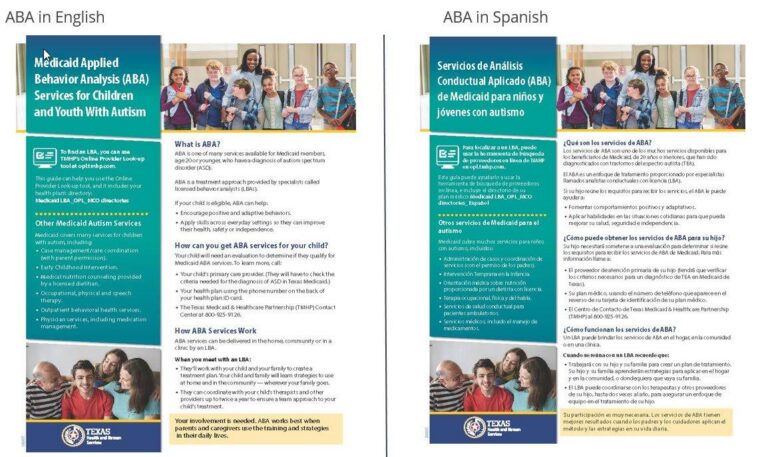
The clinical foundation is older than the app. Visual schedules and video modeling are both listed as evidence-based practices for autistic learners by the National Clearinghouse on Autism Evidence and Practice, which reviewed ninety-seven articles supporting video modeling in its 2020 update. The literature spans social skills, daily living skills, academic skills, vocational skills, and reductions in problem behavior, across age bands from early childhood through young adulthood. What is new in Hygiene Hippie is not the science. It is the delivery vehicle.
The turnover the whole industry is fighting
Conner’s premise lands harder when you put it next to the workforce data. The CDC’s Autism and Developmental Disabilities Monitoring Network reported in April 2025 that 1 in 31 eight-year-olds in the United States was identified with autism spectrum disorder in 2022, up from 1 in 36 two years earlier. Demand for ABA, OT, and adjacent supports has climbed in step. Supply has not.
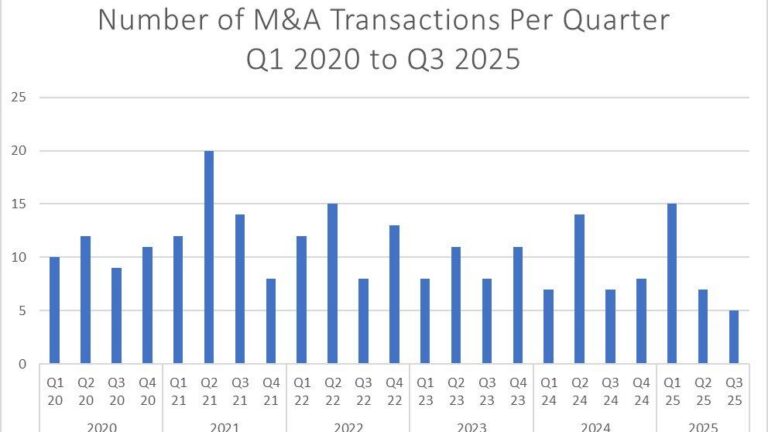
The CentralReach 2025 Autism and IDD Care Market Report puts the median annual turnover rate at ABA organizations at 65 percent, with some large operators reporting 90 to 100 percent or higher. A 2021 review in the Review Journal of Autism and Developmental Disorders documented direct-care turnover ranging from 77 to over 103 percent, meaning many organizations replace their entire frontline workforce in a single year. The Behavior Analyst Certification Board’s 2025 RBT exit survey, distributed to roughly 30,000 former RBTs whose certifications expired, identified compensation, workload, and supervisory environment as the dominant drivers.
That churn has a clinical price. Independent industry coverage cites research showing that when a client experiences two or more RBT changes in a year, measurable progress on skill acquisition can drop by more than half. The Behavior Analyst Certification Board’s Continuity of Services Toolkit treats the handoff itself as the intervention, not the paperwork around it. For a category whose value proposition rests on consistent, high-frequency delivery, a 65 to 100 percent annual turnover rate is a structural problem, not a personnel one.
Hygiene Hippie targets one slice of that structural problem: the routines that keep regressing every time the person executing them changes. It does not pretend to fix the compensation pressures or the supervisory environment. The argument is narrower. If a saved routine, with the same images and the same video model and the same step sequence, can be opened by the new RBT on day one and by the parent at home the same evening, the gap a single resignation creates gets smaller.
What Hygiene Hippie does, by Conner’s telling
On her own materials and in pilot conversations, Conner consistently emphasizes four operational features.
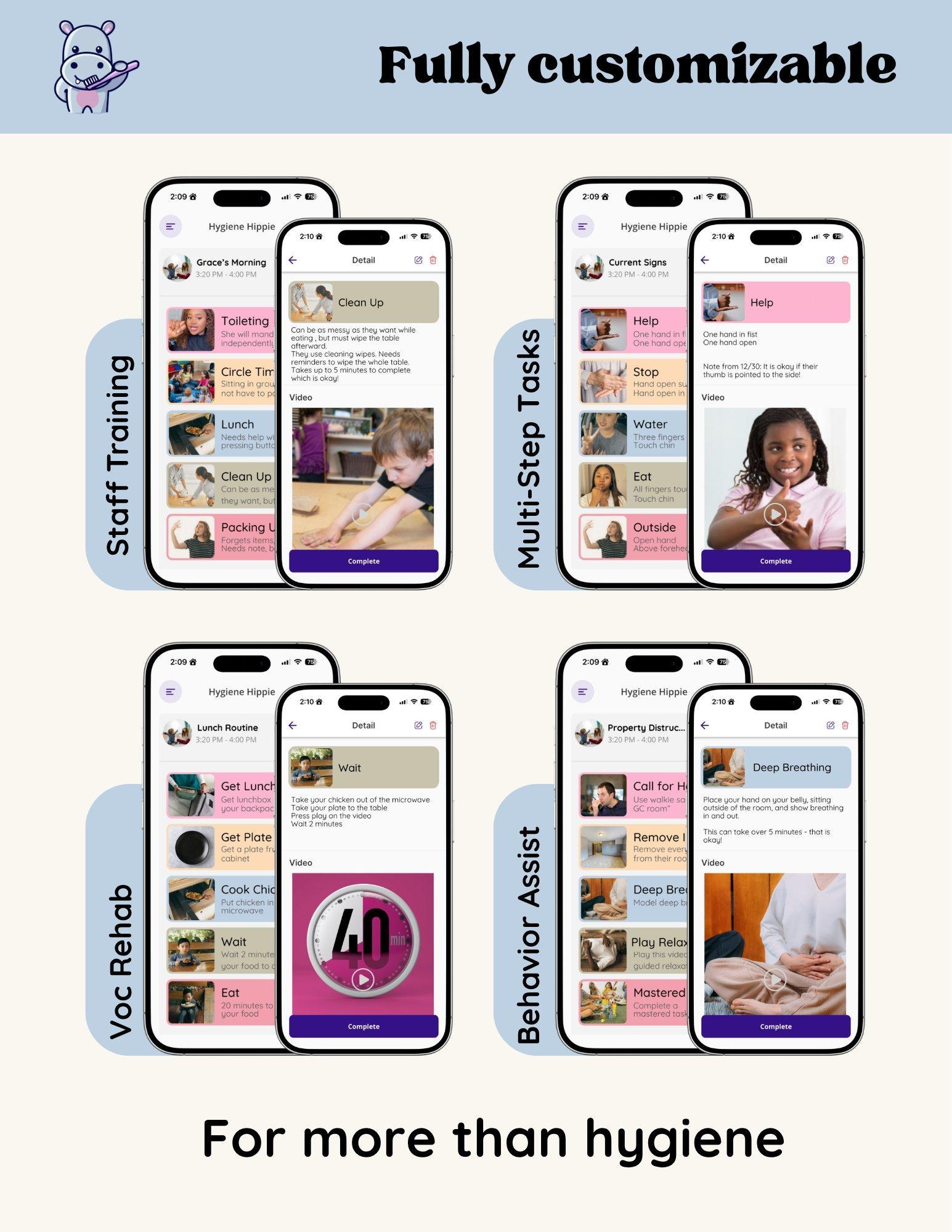
The first is the combination of visual schedules and video modeling in one customizable interface. A clinician or parent builds a routine once, using their own photos for each step and a short video model the client can replay. The two evidence-based interventions, often used separately and inconsistently, are bundled into a single saved object.
The second is the privacy architecture. No accounts. No protected health information collected. Routines live on the device. A clinic that wants to share a routine with a family does so through a code, not a credentialed login. For ABA operators that have spent the last several years navigating heavier payer scrutiny and tighter HIPAA expectations on every adjacent system they connect, a tool that simply does not collect PHI is a different procurement conversation than one that does.
The third is the scope. The app launched for hygiene because that is where Conner saw the gap most clearly in pediatric OT practice. The architecture, however, is task-agnostic. The same visual-plus-video format applies to multi-step daily living routines, to vocational tasks at supported employment sites, to the staff-training sequences a clinical lead might want every new RBT to walk through on day one, and to behavior-support sequences a BCBA designs for a specific antecedent pattern. A vocational library is in active development with supported employment providers as co-creators.
The fourth is the delivery model. Hygiene Hippie is in active thirty-day pilots with ABA clinics and residential providers in Indiana. BCBA continuing education courses are already available through OT and ABA Collab Lab, the joint education initiative Conner runs with Lindsay Watkins, BCBA, MEd, founder of NeuroBloom. The Collab Lab is BACB eligible for CEU credit, with AOTA approval pending. White-label licensing for larger ABA organizations is on offer.
What Hygiene Hippie does not claim is the part that signals the company is reading its own market accurately. Conner does not position the app as a clinical platform, a data-collection system, an electronic medical record, or a replacement for BCBA supervision. It does not capture session notes. It does not sit in the payer audit trail. It does not generate fidelity data the way a discrete trial training app might. The argument she presses, in pilots and in industry conversations, is narrower. The science behind hygiene and daily living routines in ABA is well established. The supports for delivering that science survive a staff transition. Most ABA tools have skipped that layer. Hygiene Hippie is an attempt to build for it.
From hygiene to vocational, then national
The forward plan, in Conner’s own framing, is Indiana first and national after. Version 1 of the app launched, ran in early caregiver and clinic environments, and surfaced the gaps that drove a Version 2 rebuild now active in pilots. The vocational library is the next major build, with supported employment providers serving as co-creators and early adopters rather than late customers.
The longer-term arc Conner describes is a standardization layer for any routine-based skill across any setting where staff turnover disrupts client progress. That includes ABA clinics, residential providers, supported employment, foster care, and special education. The continuing education side, run through OT and ABA Collab Lab with Lindsay Watkins, is the channel for getting BCBAs and OTs aligned on the shared language a tool like this depends on.
Whether the model holds up in outcome data is the open question every multi-disciplinary technology bet in this category has to answer. ABA has had no shortage of point solutions promising to fix a piece of the workforce problem. Most have either widened the administrative load on BCBAs or solved a billing problem rather than a delivery problem. A tool that targets the routine itself, in the hands of the person executing it, is a different category of bet, but it is still a bet.
The proof will be what the pilot data shows over the next twelve to twenty-four months. Whether a saved routine, opened by the next RBT and the parent the same evening, actually compresses the regression window the field currently treats as inevitable is the question Conner spent a decade watching nobody answer. She is, for now, the OT building the front-line delivery layer the rest of the ABA software market has yet to ship.

AT A GLANCE
| Founder & CEO: | Gracyn Conner, OTD, MS, OTR |
| Company: | Hygiene Hippie |
| Headquarters: | Indianapolis, Indiana |
| Founder background: | Pediatric OT with 10 years in and around ABA settings; Assistant Professor and Academic Fieldwork Coordinator, Department of Occupational Therapy, Marian University |
| Distinguishing feature: | Combines visual schedules and video modeling (both evidence-based practices for autism per the National Clearinghouse on Autism Evidence and Practice, 2020) into one customizable mobile platform built for the delivery layer |
| Privacy structure: | No user accounts; no PHI collected; on-device storage; routines shared via code |
| Product scope: | Hygiene routines (live); daily living, vocational, staff training, and behavior-support sequences (active or in development) |
| Active pilots: | ABA clinics, caregivers, residential providers, and vocational/supported employment programs in Indiana |
| Distribution: | Apple App Store live. Google Play Store live. Clinic pilots are currently free for the 30-day trial period. Paid access available upon pilot completion. |
| Co-founded: | OT and ABA Collab Lab with Lindsay Watkins, BCBA, MEd, founder of NeuroBloom; courses BACB eligible, AOTA approval pending |
| Industry context (turnover): | Median ABA direct-care turnover 65% in 2025; large operators reporting 90 to 100%+ (CentralReach Autism and IDD Care Market Report, 2025) |
| Industry context (prevalence): | 1 in 31 eight-year-olds identified with autism spectrum disorder in 2022 (CDC ADDM Network, MMWR April 17, 2025) |
SOURCES & REFERENCES
| 1. | Hygiene Hippie. Home, How It Works, and Who Built This pages. hygienehippie.com. Retrieved May 2026. |
| 2. | Hygiene Hippie. OT and ABA Collab Lab. hygienehippie.com/otandabacollablab. Retrieved May 2026. |
| 3. | Marian University. Faculty & Staff Directory entry: Gracyn Conner, OTD, MS, OTR, Department of Occupational Therapy, Health and Community Sciences. marian.edu/directory. Retrieved May 2026. |
| 4. | Anna Roney. “Fishers therapist creates hygiene app.” Current in Fishers (youarecurrent.com). July 16, 2025. |
| 5. | Shaw KA, Williams S, Patrick ME, et al. “Prevalence and Early Identification of Autism Spectrum Disorder Among Children Aged 4 and 8 Years: Autism and Developmental Disabilities Monitoring Network, 16 Sites, United States, 2022.” MMWR Surveillance Summaries 2025;74(SS-2):1-22. April 17, 2025. |
| 6. | CentralReach. Autism and IDD Care Market Report: 2025 Recap & 2026 Outlook. 2025. |
| 7. | BHCOE Accreditation. 2022 ABA Compensation & Turnover Report. 2022. |
| 8. | Behavior Analyst Certification Board (BACB). 2025 RBT Exit Survey, summarized in industry coverage. 2025. |
| 9. | Kirby AV, Boyd BA, Williams KL. Review on direct-care staff turnover in ABA and related human services. Review Journal of Autism and Developmental Disorders. 2021. |
| 10. | Steinbrenner JR, Hume K, Odom SL, et al. Evidence-Based Practices for Children, Youth, and Young Adults with Autism. National Clearinghouse on Autism Evidence and Practice (NCAEP), Frank Porter Graham Child Development Institute, University of North Carolina at Chapel Hill. 2020. (Lists video modeling and visual supports as evidence-based practices.) |
| 11. | Hume K, Steinbrenner JR, Odom SL, et al. “Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review.” Journal of Autism and Developmental Disorders. 2021;51(11):4013-4032. |
| 12. | Behavior Analyst Certification Board. Continuity of Services Toolkit. bacb.com. Retrieved May 2026. |