Early autism interventions with the strongest randomized trial record no longer look like drills at a table. They look like play. Naturalistic developmental behavioral interventions, or NDBIs, are play-based therapies. They retain the mechanics of applied behavior analysis but follow a child’s lead rather than an adult’s agenda. The American Academy of Pediatrics has singled them out as the intervention type with the strongest randomized-trial support for young autistic children. The field’s main evidence review lists naturalistic intervention as one of its established practices.
For practice owners and payers, the shift is not academic. It reaches into how clinicians are trained, how many therapy hours get authorized, who delivers the treatment, and what counts as medically necessary for a 2-year-old. For clinicians and organizations looking to move forward, initial steps can include seeking formal NDBI training, incorporating play-based techniques into current sessions, piloting caregiver coaching models, and connecting with peers who already use naturalistic approaches. Professional workshops, supervision, or collaborative case reviews can support the transition. These practical actions allow teams to begin adapting to best-practice models at a pace that matches their setting. It also arrives with a caveat: the strongest meta-analyses keep raising the question of how much of the measured benefit depends on who is doing the measuring.
What Counts as an NDBI
The term is newer than the practice. In 2015, Laura Schreibman and other researchers coined the term “naturalistic developmental behavioral intervention.” The goal was to unify a group of treatments that had developed separately but shared a common logic. Each blends two traditions. First are the teaching mechanics of applied behavior analysis, such as the antecedent-behavior-consequence sequence, prompting, and reinforcement. Second is developmental science, which targets skills in the order in which typically developing children acquire them.
What separates an NDBI from older behavioral models is where and how the teaching happens. Instruction is embedded in play and daily routines rather than massed at a table. The child initiates, and the adult follows the child’s lead. The reward is built into the activity itself. A child who reaches for bubbles gets bubbles—not a token or an unrelated snack. Researchers later cataloged the shared features into a fidelity measure, the NDBI-Fi, allowing a session to be scored against the model.
That contrasts with discrete trial training, the structured, adult-directed format many behavior analysts were trained on. DTT teaches in repeated, tightly controlled trials, often at a table and frequently with reinforcers unrelated to the task. It remains useful for some skills. For social communication, language, and play in very young children, contemporary research has tilted toward the naturalistic approach.
The Models With the Data
Three named models anchor the category, each with its own research program and its own developer.
The Early Start Denver Model (ESDM) was developed by Sally Rogers and Geraldine Dawson. It is the most-cited NDBI and the one with the landmark efficacy trial. In a 2010 randomized controlled trial published in Pediatrics, 48 toddlers aged 18 to 30 months received either ESDM or referral to community providers. After two years at roughly 20 hours a week, the ESDM group gained an average of 17.6 IQ points. The comparison group gained 7.0. The ESDM group also maintained its rate of growth in adaptive behavior. The result put play-based intervention on the clinical map.
JASPER was developed by Connie Kasari at UCLA. It targets the social-communication foundations that come before language: joint attention, symbolic play, engagement, and regulation. Randomized trials have tested JASPER with hundreds of children over about two decades, in Kasari’s lab and by independent groups. In one analysis, joint engagement accounted for about two-thirds of JASPER’s effect on children’s social communication. This offers a rare look at why an intervention works, not just whether it does.

Pivotal Response Treatment (PRT) was developed by Robert and Lynn Koegel. It targets “pivotal” areas, such as motivation and responsivity, based on the theory that gains in these areas spread to other skills. Multiple randomized trials have linked PRT—delivered by both clinicians and trained parents—to gains in expressive language and social communication. A 2019 trial in Pediatrics found that a PRT package improved children’s functional communication compared to treatment as usual.
The three are distinct programs, not interchangeable. Yet, what they share is the naturalistic logic and, increasingly, a delivery model that puts the parent in the room.
Two decades of randomized trials made NDBIs the most evidence-backed approach for young autistic children. Despite this, the harder question the same trials raise is how much of the gain survives when the people rating the child do not know which treatment the child received.
What the Evidence Actually Shows
The case for NDBIs rests on meta-analysis, not any single trial. A 2019 meta-analysis by Gabrielle Tiede and Katherine Walton covered 27 group-design studies. It found significant positive effects across several domains: social engagement (Hedges’ g = 0.65), overall cognition (0.48), expressive language (0.32), play (0.23), and a reduction in autism symptom severity (g = 0.38). Effects on joint attention and receptive language were smaller and only marginal. The pattern matched what the models target: social communication and language, not a fix for every feature of autism.
The endorsements followed the data. For example, the American Academy of Pediatrics, in its 2020 clinical report on autism, described NDBIs as the intervention type most supported by randomized controlled trials. Similarly, the National Clearinghouse on Autism Evidence and Practice, in its 2020 review, classified naturalistic intervention as an evidence-based practice and folded Pivotal Response Treatment into that category.
Then comes the caveat. The largest and most rigorous synthesis in the field is Project AIM. Michael Sandbank led this work, published in Psychological Bulletin in 2020. Project AIM pooled more than 1,600 effect sizes from 130 studies. It found positive effects for NDBIs in randomized trials. But when the analysis included only outcomes measured without detection bias and excluded parent-reported outcomes, the significant effects largely disappeared. A 2023 update reached the same conclusion. It warned that adverse events, like increased child distress and parent stress, were poorly tracked across the literature.
The implication is not that NDBIs do not work. A meaningful share of the measured benefit comes from outcomes rated by unblinded parents who knew their child was being treated. This is a recognized source of inflation in intervention research. For payers and clinicians deciding what to authorize and what to promise families, that distinction matters.
The Caregiver-Mediated Turn
The newest move in the field is not a new model but a new deliverer: the parent. Caregiver-mediated NDBIs train a parent to use intervention strategies during everyday interactions. A clinician coaches rather than delivers. Project ImPACT was developed by Brooke Ingersoll. It is the most widely disseminated example and was recognized by the national evidence clearinghouse as a manualized intervention meeting criteria.
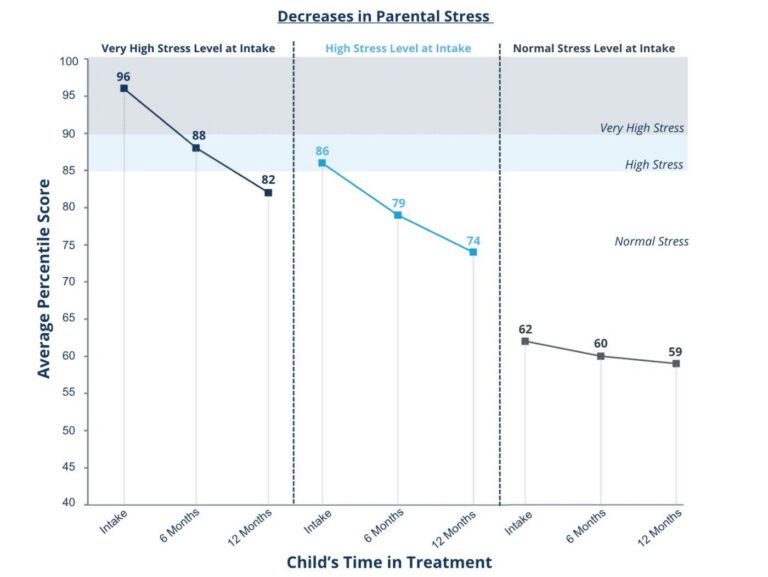
The appeal is part clinical and part economic. Controlled trials have linked parent-mediated NDBIs to better parent implementation, higher parent self-efficacy, and lower parenting stress. They also extend intervention into hours when a clinician is not present. Parent-mediated NDBIs travel well over telehealth, which expanded sharply after 2020. Coaching has become more accessible to families far from a clinic, including Medicaid-enrolled families in under-resourced areas.
The billing system already has a place for this. Caregiver coaching maps onto CPT 97156, the family adaptive behavior treatment guidance code. This is separate from 97153, the code for direct one-to-one therapy delivered by a technician. Payer adoption of telehealth for these caregiver-guidance codes has widened since the pandemic. Coverage still varies by state and plan. For a sector under pressure on staffing and direct-therapy hours, a model that shifts some delivery to trained parents and bills under an existing code is more than a clinical preference.
Beyond the 40-Hour Model
The naturalistic turn runs into one of the industry’s oldest assumptions: more hours are better. The benchmark of 25 to 40 hours a week traces to early intensive behavioral intervention research from the 1980s. A 2021 multisite randomized trial led by Rogers and colleagues, published in the Journal of the American Academy of Child and Adolescent Psychiatry, tested that assumption head-on. The study assigned 87 toddlers to early intensive behavioral intervention or ESDM, at 15 or 25 hours a week. It found no significant difference in outcomes by intervention style or intensity.
One trial does not settle a decades-old debate, and the sample was small. This finding comes at a sensitive moment. Payers are scrutinizing high-hour authorizations. Providers ask whether the 40-hour workweek is based on evidence or habit. If a lower-intensity, play-based model produces similar results, the clinical and financial case for maximal hours weakens.
When 15 hours a week of play-based therapy matches 25 hours of intensive intervention, the question of how many hours to authorize stops being purely clinical.
The Implementation Gap
Endorsement has outpaced adoption. Many board-certified behavior analysts were trained on discrete trial methods and have had little formal exposure to NDBIs. A 2024 study in Behavior Analysis in Practice on barriers to NDBI adoption in ABA settings found that clinicians had to unlearn DTT habits, often lacked training and confidence in the naturalistic approach, held mixed attitudes toward it, and ran into organizational constraints. Access to the branded, manualized programs is itself uneven.
There is movement to close the gap, including proposals to build NDBI content into BCBA training rather than treat it as a post-credential specialty. The shift also fits a broader reckoning over assent-based and compassionate care. Following a child’s lead and embedding learning in preferred activities answers some of the neurodiversity movement’s objections to rigid, adult-directed therapy, a case made directly in a 2022 paper framing NDBIs as a bridge between early intervention and neurodiversity perspectives.
The evidence base is still being built. A caregiver-coaching NDBI trial at the University of Texas at Austin is recruiting now, with primary results expected in 2026, and a larger caregiver-coaching trial is underway in Cape Town. Those results will arrive as payers and BCBA training programs decide how fast to move, making 2026 a test of whether the naturalistic turn becomes the field’s default or stalls at endorsement.
AT A GLANCE
| What NDBIs are: | Play-based therapies blending ABA teaching mechanics with developmental sequencing; term coined by Schreibman et al., 2015 |
| Core models: | Early Start Denver Model, JASPER, Pivotal Response Treatment, Project ImPACT (caregiver-mediated) |
| ESDM landmark trial: | Gained 17.6 IQ points vs 7.0 in the comparison group after 2 years (Dawson et al., Pediatrics, 2010) |
| Meta-analysis effects: | Social engagement g = 0.65, cognition 0.48, expressive language 0.32 (Tiede & Walton, Autism, 2019) |
| Strongest RCT support: | NDBIs called the intervention type most supported by RCTs (AAP clinical report, 2020) |
| The key caveat: | Significant effects largely vanish without parent-report and unblinded outcomes (Project AIM / Sandbank et al., 2020; 2023 update) |
| Dose finding: | 15 vs 25 hours a week, and ESDM vs EIBI, showed no significant outcome difference (Rogers et al., JAACAP, 2021) |
| Caregiver billing: | Coaching maps to CPT 97156, family adaptive behavior treatment guidance |
| Adoption barrier: | Many BCBAs trained on DTT, with limited NDBI training and confidence (Behavior Analysis in Practice, 2024) |
| Trials to watch: | UT Austin caregiver-coaching NDBI (NCT06923553), results due 2026; ACACIA trial, Cape Town |
SOURCES & REFERENCES
| 1. | Schreibman L, Dawson G, Stahmer AC, et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J Autism Dev Disord. 2015;45(8):2411–2428. doi:10.1007/s10803-015-2407-8 |
| 2. | Frost KM, Brian J, Gengoux GW, et al. Identifying and measuring the common elements of naturalistic developmental behavioral interventions: Development of the NDBI-Fi. Autism. 2020;24(8):2285–2297. doi:10.1177/1362361320944011 |
| 3. | Dawson G, Rogers S, Munson J, et al. Randomized, Controlled Trial of an Intervention for Toddlers With Autism: The Early Start Denver Model. Pediatrics. 2010;125(1):e17–e23. doi:10.1542/peds.2009-0958 |
| 4. | Kasari C, Freeman S, Paparella T. Joint attention and symbolic play in young children with autism: a randomized controlled intervention study. J Child Psychol Psychiatry. 2006;47(6):611–620. doi:10.1111/j.1469-7610.2005.01567.x |
| 5. | Kasari Lab, University of California, Los Angeles. JASPER: program overview and randomized-trial summary. jaspertraining.org. Accessed June 2026. |
| 6. | Gengoux GW, Abrams DA, Schuck R, et al. A Pivotal Response Treatment Package for Children With Autism Spectrum Disorder: An RCT. Pediatrics. 2019;144(3):e20190178. doi:10.1542/peds.2019-0178 |
| 7. | Tiede G, Walton KM. Meta-analysis of naturalistic developmental behavioral interventions for young children with autism spectrum disorder. Autism. 2019;23(8):2080–2095. doi:10.1177/1362361319836371 |
| 8. | Sandbank M, Bottema-Beutel K, Crowley S, et al. Project AIM: Autism Intervention Meta-Analysis for Studies of Young Children. Psychol Bull. 2020;146(1):1–29. doi:10.1037/bul0000215 |
| 9. | Sandbank M, Bottema-Beutel K, Crowley S, et al. Autism intervention meta-analysis of early childhood studies (Project AIM): updated systematic review and secondary analysis. 2023. |
| 10. | Hyman SL, Levy SE, Myers SM; AAP Council on Children With Disabilities, Section on Developmental and Behavioral Pediatrics. Identification, Evaluation, and Management of Children With Autism Spectrum Disorder. Pediatrics. 2020;145(1):e20193447. doi:10.1542/peds.2019-3447 |
| 11. | Steinbrenner JR, Hume K, Odom SL, et al. Evidence-Based Practices for Children, Youth, and Young Adults With Autism. National Clearinghouse on Autism Evidence and Practice, Frank Porter Graham Child Development Institute, University of North Carolina at Chapel Hill. 2020. |
| 12. | Ingersoll B, et al. Telehealth coaching in Project ImPACT indirectly affects children’s expressive language through parent strategy use: a randomized controlled trial. Autism Research. 2024. doi:10.1002/aur.3230 |
| 13. | Rogers SJ, Yoder P, Estes A, et al. A Multisite Randomized Controlled Trial Comparing the Effects of Intervention Intensity and Intervention Style on Outcomes for Young Children With Autism. J Am Acad Child Adolesc Psychiatry. 2021;60(6):710–722. doi:10.1016/j.jaac.2020.06.013 |
| 14. | The Challenges Associated With Changing Practice: Barriers to Implementing Naturalistic Developmental Behavioral Interventions in ABA Settings. Behavior Analysis in Practice. 2024. doi:10.1007/s40617-024-01011-2 |
| 15. | Schuck RK, Tagavi DM, Baiden KMP, et al. Neurodiversity and Autism Intervention: Reconciling Perspectives Through a Naturalistic Developmental Behavioral Intervention Framework. J Autism Dev Disord. 2022;52:4625–4645. doi:10.1007/s10803-021-05316-x |
| 16. | ClinicalTrials.gov. Implementation of Naturalistic Developmental Behavioral Intervention (NDBI) Through Coaching Caregivers of Young Autistic Children. NCT06923553. University of Texas at Austin. 2025. |
| 17. | Autism Caregiver Coaching in Africa (ACACIA): protocol for a type 1 hybrid effectiveness-implementation trial. 2024. |
| 18. | American Medical Association Current Procedural Terminology; ABA Coding Coalition. Adaptive behavior services codes 97153 and 97156. abacodes.org. Accessed June 2026. |