
One Billing Rule Change, One Child Discharged
HARTFORD, VERMONT — Sam was supposed to continue ABA therapy for another six months. The 6-year-old with profound autism had gone from non-speaking and withdrawn to doing puzzles, playing with peers, and communicating basic needs through a Picture Exchange Communication System. His mother, Jennifer Beane-Edgar, described the change as immeasurable. Then, in February 2026, the clinic told her Sam was being discharged early.
The reason was not clinical. Sam’s ABA provider had spent January and February watching its Medicaid revenue fall roughly 16 percent as a result of a billing rule change that took effect January 1, 2026. The clinic began discharging half of its Medicaid clients to stay financially viable. Sam was among them.
The change came from the Department of Vermont Health Access, which administers the state’s Medicaid program. Starting in 2026, Vermont Medicaid no longer allows ABA providers to bill for both the behavior technician’s time and the supervising BCBA’s time when both are working with the same child at the same time. That practice, known as concurrent billing of CPT codes 97153 and 97155, had been a standard part of how Vermont ABA clinics were reimbursed. Now it is not.
Vermont is not doing something unusual in the national landscape. It is doing something that many states have not yet done: defining its policy clearly in writing, under pressure from federal auditors who found that Wisconsin had done the same thing Vermont was doing and had charged the federal government $18.5 million for it. Vermont says it is protecting itself from a similar finding. Its ABA providers say the protection is coming out of their operating budgets, and by extension, out of their clients’ therapy hours.
“Honestly, the structure of our work is too complex for a behavior technician to do with fidelity, the way it should be done, without BCBA oversight. We’re ethically required to provide services in that structure. You have to have two people there for a portion of the time to make sure it’s done right.” — Cortney Keene, BCBA, Founder, Keene Perspectives (VTDigger, March 2026)
The Billing Math: Where the Revenue Goes

To understand what Vermont changed and why it matters, the billing mechanics need to be clear. ABA therapy operates on time-based CPT codes billed in 15-minute units. The two codes at the center of this dispute are: CPT 97153, which covers adaptive behavior treatment delivered by a behavior technician under BCBA supervision, and CPT 97155, which covers treatment with protocol modification delivered directly by a qualified healthcare professional, typically a BCBA, which can include simultaneous direction of a technician.
Under the old Vermont system, ABA therapy companies could bill as follows: if a child received 10 hours of ABA services in a week, and a BCBA was present for 2 of those 10 hours observing and directing the behavior technician, the clinic could submit 10 hours of 97153 and 2 hours of 97155 for a total of 12 billable hours. The BCBA time was additive to the technician time, not a replacement for it.
Under the new Vermont system, that same 10-hour week generates 10 billable hours, period. The BCBA’s presence during those 2 hours is not separately reimbursable. Vermont Medicaid’s reasoning, laid out in its February 5, 2026 presentation to the Vermont House Health Care Committee, is that there is one child and one hour of face-to-face care. Billing two codes for that one hour means billing twice for the same unit of time, which is prohibited under the 2023 American Medical Association CPT coding guidelines.
The DVHA presentation put it plainly: “billing both codes at the same time for the same child does not meet national American Medical Association coding standards.” Vermont cited 2023 AMA CPT guidance specifying that Medicaid can only reimburse for the child’s face-to-face time receiving services, and that two clinicians cannot bill for the same time period with one child.
The providers’ counterargument: Cortney Keene at Keene Perspectives and Celia O’Flaherty at Little Royals Early Intervention Center in Williston both maintain that two different clinicians are providing two different services. The behavior technician is implementing the protocol. The BCBA is modifying it, monitoring it, and providing real-time feedback. Those are not the same task. Eliminating payment for the BCBA’s time does not eliminate the clinical requirement for the BCBA’s presence. The oversight work happens regardless. It just no longer gets paid.
The ABA Coding Coalition, the national body that publishes guidance on ABA CPT codes, submitted written comments to DVHA when the policy was proposed in late 2025. The Coalition’s own FAQ states that 97153 and 97155 can be billed concurrently “as long as the criteria in the descriptors of both codes are met.” The tension between that guidance and Vermont’s reading of the 2023 AMA update is the substantive dispute underlying the revenue figures.
Why Wisconsin Put Vermont on Alert
Vermont did not act in a vacuum. The policy change was a direct response to a federal Office of Inspector General audit that published its findings on Wisconsin in July 2025. That report found that Wisconsin had made at least $18.5 million in improper fee-for-service Medicaid payments for ABA services provided to children diagnosed with autism in 2021 and 2022. All 100 sampled enrollee-months in the audit contained at least one improper or potentially improper claim line.
Concurrent billing of 97155 and 97153 in the absence of a clear written policy was identified as a key deficiency. OIG recommended that Wisconsin refund $12.2 million to the federal government and conduct periodic statewide post-payment reviews.
Wisconsin was not alone. In a prior audit, OIG found that Indiana had made at least $56 million in improper Medicaid ABA payments for 2019 and 2020. In March 2024, the Massachusetts Inspector General published a report finding up to $17.3 million in ABA overpayments. The pattern across all three states was similar: inadequate supervision documentation, concurrent billing without clear policy, session notes that did not support the units billed.
Vermont’s DVHA, reviewing its own program, identified a specific vulnerability: the state had no written policy on concurrent ABA billing. Without a written policy, Vermont had no defensible position if OIG came to audit. DVHA’s February 2026 legislative presentation stated the objective directly: “To protect Vermont from similar findings and potential multimillion-dollar liabilities for the state and providers, DVHA must clearly define its ABA concurrent billing policy.”
The timing matters. Under the Trump administration, the federal government has increased its scrutiny of how states spend Medicaid dollars. Vermont is simultaneously managing a separate Congressional inquiry into Medicaid fraud, waste, and abuse in the state, as reported by VTDigger in March 2026. ABA was the primary area where DVHA identified active vulnerability.
Vermont had no written concurrent billing policy for ABA services before January 2026. Without one, the state had no defensible position if the OIG audited it. Wisconsin’s $18.5 million finding was the example Vermont was explicitly trying to avoid.
The Real-World Impact
Vermont’s DVHA projected, based on its own modeling, an average 12 percent decrease in billable hours per provider. The two clinics that have spoken publicly on the record are experiencing worse than the projected average.
At Keene Perspectives in Hartford, revenue dropped approximately 16 percent in January and February. Cortney Keene and her husband Chris Keene, both BCBAs, have already begun discharging half of their Medicaid clients. Sam, Jennifer Beane-Edgar’s son, was among the children let go six months before his planned transition to public school.
At Little Royals Early Intervention Center in Williston, clinical director Celia O’Flaherty reported a 17 percent overall income drop. The per-client impact is not uniform: some clients generate a 15 percent revenue reduction under the new rules while others generate a 50 percent reduction, depending on how much BCBA time was previously being separately billed for each case. “The 50% feels staggering to us,” O’Flaherty told VTDigger. The variance reflects how heavily each clinic relied on concurrent billing for specific clients. For clinics serving children with higher support needs, those who require more frequent protocol modification and more intensive BCBA presence, the exposure is greatest.
Little Royals has not yet discharged Medicaid clients. O’Flaherty is pursuing alternative revenue sources, including contracting clinicians with school districts. But both she and the Keenes told VTDigger they are aware of Vermont ABA clinics already evaluating whether to close entirely. Neither named those clinics publicly.
Vermont Medicaid serves 320 unique ABA members. That is a small number by most states’ standards. But the density of those 320 children across Vermont’s rural geography means losing even one or two clinics removes access not just for that clinic’s clients but for every family in the surrounding area who has nowhere else to go.
The Rate Study Is the Off-Ramp
Both sides of this dispute point to the same potential resolution. Vermont passed Act 14 in 2025, which requires DVHA to conduct a formal ABA rate study before July 2026. The rate study will evaluate whether current Medicaid payment rates for ABA services are adequate to support statewide access.
Grace Johnson, a Medicaid policy analyst at the Vermont Agency of Human Services, described the rate study as the appropriate mechanism for addressing provider revenue concerns. “If the reimbursement that was happening was insufficient, the rate study would address that,” she said. DVHA’s position is that the concurrent billing change is a compliance correction, not a rate cut. If the base rates turn out to be too low to sustain providers after the compliance correction takes effect, the answer is raising the base rates, not restoring a billing practice the state considers improper.
O’Flaherty at Little Royals shares that view, conditionally. “If this is our new reality, then there needs to be a rate change,” she said. The condition is the operative part. She is not accepting the concurrent billing ban as the permanent baseline. She is accepting it as the current reality while the rate study proceeds, and banking on the rate study producing an adjustment that makes the new billing rules financially workable.
The rate study will include extensive provider engagement, according to the DVHA legislative presentation. Its scope, timeline, and methodology have not been publicly detailed as of this writing. Whether it will be completed before July 2026, and whether its findings will translate into a rate increase that actually compensates for the lost concurrent billing revenue, are open questions. Alex McCracken, a spokesperson for DVHA, said the department would continue to monitor how providers respond to the billing changes through 2026.
The risk in the interim is that providers do not wait for the rate study. Clinic closures and client discharges are happening now. A rate study completed in June 2026 cannot undo six months of service disruption for children who needed continuous therapy in January, February, and March.
The National Tripwire
Vermont is the clearest recent example of a dynamic that is building across the country: federal ABA billing enforcement is pushing state Medicaid programs to tighten the policies they have let remain ambiguous for years. Vermont’s situation is not the exception. It is the preview.
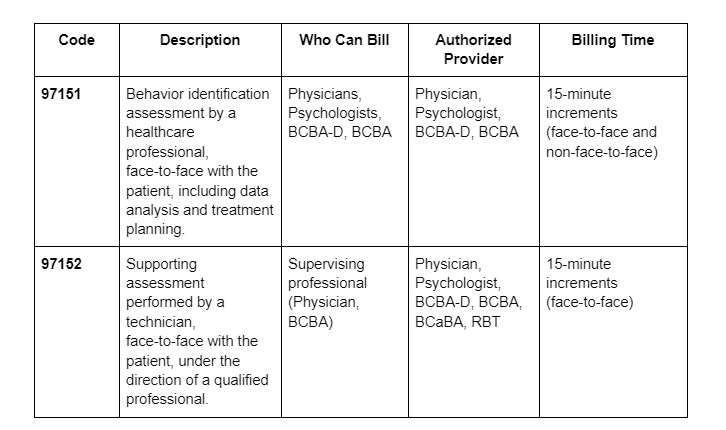
The OIG has now audited Wisconsin and Indiana on ABA billing and found significant improper payments in both states. Massachusetts has had a comparable state-level finding. The ABA Coding Coalition tracks payer interactions across the country and has engaged not only with Vermont but with Virginia around concurrent billing of 97151 and 97153, and with Blue Cross Blue Shield of Michigan around documentation restrictions on 97153. The enforcement conversations are happening in multiple places at once.
The specific question of whether 97153 and 97155 can be billed concurrently does not have a uniform national answer. The ABA Coding Coalition says yes, when the criteria of both code descriptors are met. The 2023 AMA CPT guidance says Medicaid can only reimburse for child face-to-face time, and that two clinicians cannot bill for the same time period. Vermont has read that guidance as prohibiting concurrent billing. Other state Medicaid programs have not yet clarified their position.
Any state Medicaid program that currently allows concurrent billing of 97153 and 97155 without a documented written policy is sitting in the same position Vermont was in before November 2025. If OIG audits that state and finds the same pattern it found in Wisconsin, the outcome will be similar: a finding of improper payments, a recommended federal repayment, and a mandate to establish a written policy. The only difference is whether the state gets to define that policy proactively, before the audit, or reactively, after it.
For ABA practice owners and operators in Medicaid-participating organizations, that timing question is not abstract. If your state Medicaid program does not have a written concurrent billing policy, the safest assumption is that one is coming. The question is whether it arrives through a proactive process that includes provider input and a rate adjustment, the way Vermont’s was supposed to work, or through an enforcement action that leaves no runway.
AT A GLANCE
| Policy change effective: | January 1, 2026 (announced November 10, 2025) |
| Issuing agency: | Department of Vermont Health Access (DVHA), Vermont Agency of Human Services |
| Change: | Prohibited concurrent billing of CPT 97153 (behavior tech treatment) and CPT 97155 (BCBA protocol modification) for same child same time period |
| Basis cited: | 2023 AMA CPT guidance; OIG Wisconsin finding; absence of written VT policy |
| DVHA projected impact: | 12% average decrease in billable hours per provider |
| Actual reported impact: | Keene Perspectives: 16% revenue drop (Jan-Feb 2026); Little Royals: 17% overall, 15%-50% per client |
| Vermont ABA Medicaid members: | 320 unique members served in 2025 (DVHA, February 2026) |
| Vermont ABA providers: | Approximately 20; roughly half are clinic-based |
| Wisconsin OIG finding: | $18.5 million improper ABA FFS payments (2021-2022); concurrent billing without written policy was a key deficiency (OIG, July 2025) |
| Indiana OIG finding: | $56 million improper ABA payments (2019-2020) |
| Massachusetts finding: | Up to $17.3 million in ABA overpayments (MA Inspector General, March 2024) |
| Rate study deadline: | Before July 2026 (required by Act 14); includes provider engagement |
| DVHA position on fix: | “If access issues arise, rates are the appropriate remedy” |
| ABA Coding Coalition position: | 97153 and 97155 can be billed concurrently when criteria of both code descriptors are met (abacodes.org FAQ) |
SOURCES & REFERENCES
| 1. | Gieger, Olivia. “Some Kids With Autism Are Losing Therapy Services After a Medicaid Change Reduces Clinics’ Revenue.” VTDigger. March 30, 2026. https://vtdigger.org/2026/03/30/some-kids-with-autism-are-losing-therapy-services-after-a-medicaid-change-reduces-clinics-revenue/ |
| 2. | Gieger, Olivia. “Some Kids With Autism Are Losing Therapy Services After a Medicaid Change Reduces Clinics’ Revenue.” Valley News (via VTDigger). April 7, 2026. https://vnews.com/2026/04/07/vermont-medicaid-aba-billing-changes/ |
| 3. | Gieger, Olivia. “Centers for Children With Autism Fear Proposed Medicaid Changes May Threaten Ability to Operate.” VTDigger. December 19, 2025. https://vtdigger.org/2025/12/19/centers-for-children-with-autism-fear-proposed-medicaid-changes-may-threaten-ability-to-operate/ |
| 4. | Groves, DaShawn. “Applied Behavior Analysis (ABA) Changes.” Presentation to Vermont House Health Care Committee. February 5, 2026. https://legislature.vermont.gov/Documents/2026/Workgroups/House%20Health%20Care/Miscellaneous/W~DaShawn%20Groves~ABA%20Presentation~2-5-2026.pdf |
| 5. | Department of Vermont Health Access. “VT Medicaid Applied Behavior Analysis Coding Updates.” November 10, 2025. https://dvha.vermont.gov/sites/dvha/files/documents/VT_Medicaid_ABA_Coding_Updates_20251110.pdf |
| 6. | U.S. Department of Health and Human Services, Office of Inspector General. “Wisconsin Made at Least $18.5 Million in Improper Fee-For-Service Medicaid Payments for Applied Behavior Analysis Provided to Children Diagnosed With Autism.” Report A-06-23-01002. July 2025. https://oig.hhs.gov/reports/all/2025/wisconsin-made-at-least-185-million-in-improper-fee-for-service-medicaid-payments-for-applied-behavior-analysis-provided-to-children-diagnosed-with-autism/ |
| 7. | Meier, Daniel, and Cassie Gawron Sikorski. “OIG Finds Significant Improper Medicaid Payments for ABA Services in Wisconsin and Indiana.” Benesch, Friedlander, Coplan & Aronoff LLP. January 9, 2026. https://www.beneschlaw.com/insight/oig-finds-significant-improper-medicaid-payments-for-aba-services-in-wisconsin-and-indiana-signaling-greater-enforcement-efforts-for-aba-on-the-horizon/ |
| 8. | ABA Coding Coalition. “Letters in Support of ABA Providers.” abacodes.org. Accessed April 2026. https://abacodes.org/aba-coding-coalition-letters-in-support-of-aba-providers/ |
| 9. | ABA Coding Coalition. “Frequently Asked Questions.” abacodes.org. Accessed April 2026. https://abacodes.org/frequently-asked-questions/ |
| 10. | Gieger, Olivia. “Vermont Targeted in Federal Investigation of Medicaid Waste, Fraud and Abuse.” VTDigger. March 6, 2026. https://vtdigger.org/2026/03/06/vermont-targeted-in-federal-investigation-of-medicaid-waste-fraud-and-abuse/ |









