The Last State Standing
AUSTIN, TEXAS — On February 1, 2022, Texas became the 50th state in the United States to cover Applied Behavior Analysis therapy through its Medicaid program. The milestone was eight years in the making. In July 2014, the Centers for Medicare and Medicaid Services had issued the informational bulletin clarifying that states were required, under EPSDT, to cover medically necessary autism services for Medicaid-eligible children under 21. California implemented coverage within months. Most states followed within a few years. Texas took until 2022.
The delay was not accidental. Texas runs one of the largest and most complex Medicaid programs in the country — serving approximately 5.4 million people, predominantly children and the elderly — and its political leadership had shown limited enthusiasm for expanding Medicaid benefits of any kind. The ABA benefit arrived only after years of sustained advocacy by the Autism Society of Texas, the Texas Association for Behavior Analysis Public Policy Group, Autism Speaks, and families across the state who had been paying out of pocket for services that federal law had long required Medicaid to cover.
The legislative pathway ran through multiple sessions. In 2007, HB 1919 established commercial insurance coverage for children ages two to six with autism. SB 1484 in 2013 removed the age cap for diagnosis but imposed a $36,000 annual benefit limit for children over ten. SB 589 established state licensure for behavior analysts — a prerequisite for Medicaid enrollment. The Medicaid benefit itself was authorized through HB 1’s Rider 32 in the 86th Legislature (2019), which directed the Health and Human Services Commission to add ABA as a covered benefit under the Texas Health Steps Comprehensive Care Program. Implementation was delayed by COVID-19 and administrative complexity. When it finally launched, Texas chose a delivery model that would define every problem that followed: managed care.
The Managed Care Decision: How Texas Structured the Benefit

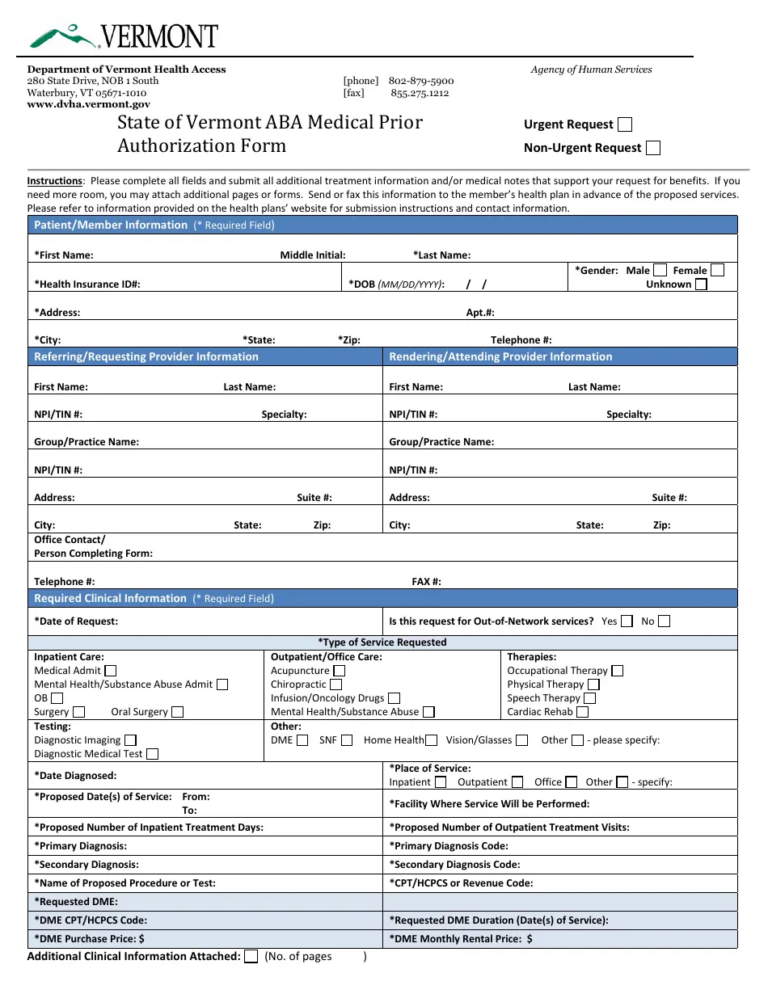
Unlike states that administered ABA through fee-for-service Medicaid — where providers bill the state directly at published rates — Texas routed its entire ABA benefit through Managed Care Organizations. Under this structure, HHSC sets baseline fee-for-service rates, but MCOs contract separately with individual providers and may negotiate different reimbursement terms. Families enrolled in Medicaid are assigned to one of several MCOs depending on their geographic service delivery area, and they can only receive ABA services from providers who are credentialed with their specific MCO.
The MCOs administering ABA in Texas include some of the largest managed care companies in the country: Superior HealthPlan, Amerigroup, UnitedHealthcare Community Plan, Molina Healthcare, Blue Cross Blue Shield of Texas, Texas Children’s Health Plan, Parkland Community Health Plan, and others depending on the service area. Each MCO maintains its own provider network, its own credentialing process, its own prior authorization requirements, and its own interpretation of medical necessity criteria — even though all are nominally implementing the same HHSC-published policy.
The result was structural fragmentation from the first day of implementation. A provider who wanted to serve Medicaid families had to enroll with TMHP (the state’s claims administrator), then separately credential with every MCO in their service area. Each credentialing process could take up to 180 days. A Licensed Behavior Analyst in Houston might need to credential with four or five MCOs before they could see the full range of Medicaid families walking through their door. In the meantime, those families were on waitlists.
“The reimbursement rates for ABA under the Medicaid benefit have not been high enough for many providers to be able to take clients on Medicaid. In addition, the process to become a Medicaid/ABA provider has been long and challenging. These factors have led to a slower rollout of the ABA benefit and a lack of therapy providers.” — Autism Society of Texas, 2023
The Rate Problem: Too Low to Operate
The rates HHSC set for ABA services were, from the beginning, a source of provider frustration. Texas Medicaid uses a resource-based fee methodology that applies a conversion factor to relative value units. The conversion factor for children’s services was approximately $28.07 — significantly below what commercial insurance typically pays for the same CPT codes. For the most common ABA procedure code — 97153, adaptive behavior treatment by protocol, the bread-and-butter code for direct therapy delivered by a behavior technician — the resulting per-unit rate was far below what providers needed to cover wages, supervision, overhead, and the administrative burden of Medicaid compliance.
The practical effect was predictable. Many ABA providers, including some of the largest companies in the state, chose not to credential with Medicaid at all. Others credentialed selectively, accepting only certain MCOs or capping the number of Medicaid clients they would serve. Families with Medicaid coverage had a legal right to ABA services under EPSDT. What they did not have was a provider willing to accept the rate Medicaid was paying.
The problem compounded over time. The November 2024 release of the 2025 Medicaid fee schedule included a 2.83 percent reduction in the conversion factor — following five consecutive years of payment reductions. While the cuts applied across Medicaid services broadly, the effect on ABA providers was particularly acute because the rates had started low and the cumulative erosion had not been offset by the kind of emergency legislative rate increases that other states (such as Colorado in 2023) had implemented.

The Provider Landscape: A State With Everything and Not Enough
Texas is, by most measures, the single most important state in the ABA industry. It is the headquarters of Action Behavior Centers, the largest ABA provider in the country. Behavioral Innovations, with more than 100 clinics, has 63 of them in Texas. BlueSprig Pediatrics, the KKR-backed platform, launched in Houston. RethinkFirst built its platform serving Texas providers. According to the Behavior Analyst Certification Board, nearly 4,000 BCBAs were certified in Texas as of mid-2024 — one of the largest concentrations in the country.
And yet, for families on Medicaid, the abundance is an illusion. The providers are there. Many of them simply do not accept Medicaid. Texas Children’s Health Plan, one of the state’s largest MCOs, publicly acknowledged the gap by temporarily covering services from out-of-network providers while it worked to grow its in-network ABA panel. Behavioral Innovations began accepting select MCOs and posted guidance for families navigating the waitlist process. The Autism Society of Texas set up a dedicated email address for families unable to find Medicaid ABA providers and used the reports to build their legislative advocacy case.
The scale of unmet need is difficult to quantify precisely because Texas does not publicly report how many children are receiving Medicaid-funded ABA, how many are on waitlists, or what the average wait time is. The Autism Society of Texas has called for HHSC to collect and share this data — including spending per client, number of children served per year, and a breakdown by MCO — as a condition of continued funding. As of the 89th Legislature, that transparency requirement had not been enacted.
The Legislative Response: The 89th Session and Beyond
The 89th Texas Legislature convened on January 14, 2025 and concluded on June 2, 2025. Autism advocacy organizations entered the session with a clear set of priorities: $70 million per year in additional general revenue funding for the Medicaid ABA program, a reporting mechanism to track spending and access, and the creation of an advisory committee to address problems with the benefit’s implementation.
The broader Medicaid budget context was formidable. HHSC requested $9.2 billion in additional funding, with most of it going to cover Medicaid cost growth. The overall state budget allocated $82.3 billion to Medicaid — a figure that reflected both rising enrollment and medical inflation. ABA competed for attention alongside dozens of other Medicaid priorities, from nursing facility rates to Early Childhood Intervention funding to Medicaid waiver waitlists that stretch years.
The legislature did approve an $18 million increase for Early Childhood Intervention — the program that identifies developmental delays in infants and toddlers and is often the first step toward an autism diagnosis and eventual ABA referral. It also invested in overhauling the state’s Medicaid and SNAP technology systems. But the specific ABA rate increases and transparency requirements the autism community had sought were not among the session’s final outcomes. HB 564, introduced in the 89th session to address health benefit plan coverage for autism spectrum disorders, was referred to the Insurance Committee on March 3, 2025 but did not advance.
“Improved funding & transparency for the Autism Medicaid Services Program to meet the extensive needs of children and young adults with Autism. Allocate $70 million in general revenue per year. Ensure that HHSC collects and shares data on how much is being spent on the program, how many children and young adults are being served per year, and the costs per client.” — Autism Society of Texas, 89th Legislature advocacy priorities

The National Template: Why Texas Matters for Every State
Texas’s experience with Medicaid ABA is not just a Texas story. It is a preview of what happens when the largest-population states bring ABA into managed care — and what the consequences are when rates are set below market, credentialing is slow, and oversight is limited. The same dynamics that have produced provider shortages and family waitlists in Texas are now playing out in Arizona (where MCO contract terminations removed the two largest providers from the Mercy Care network), in Indiana (where a 2,800 percent spending increase produced an HHS OIG audit finding $56 million in improper payments), and in Nebraska (where a 48 percent rate cut threatened to push providers out of the state entirely).
The managed care model is not inherently the problem. Managed care can, in theory, provide better care coordination, utilization management, and cost control than fee-for-service. But when MCOs are given the authority to set provider rates and manage networks without adequate state oversight of access and network adequacy, the result is a system where the legal right to services under EPSDT coexists with the practical inability to access them. Texas, as the last state to implement the benefit and the first to do so entirely through managed care, is the most visible laboratory for whether that model can work for ABA.
The answer, three years in, is that it has not worked well enough. The families who fought for a decade to get ABA covered under Texas Medicaid now have the coverage. What they do not yet have — in too many cases — is the care.
AT A GLANCE
State: Texas
Medicaid ABA Effective: February 1, 2022 (50th and final state to implement)
Delivery Model: 100% managed care — ABA delivered exclusively through MCOs, not fee-for-service
Program: Texas Health Steps Comprehensive Care Program (THSteps-CCP); EPSDT benefit for Medicaid enrollees under 21 with ASD
Key MCOs: Superior HealthPlan, Amerigroup, UnitedHealthcare Community Plan, Molina, BCBS of Texas, Texas Children’s Health Plan, Parkland Community Health Plan
Legislative History: HB 1919 (2007, commercial coverage ages 2–6); SB 1484 (2013, removed age cap, $36K cap over 10); SB 589 (BCBA licensure); HB 1 Rider 32 (86th Leg., 2019, authorized Medicaid benefit)
BCBAs in Texas: ~4,000 certified (BACB, mid-2024)
Conversion Factor: ~$28.07 for children’s services; 2.83% reduction in 2025 fee schedule after 5 consecutive years of cuts
Credentialing Time: Up to 180 days per MCO; providers must credential separately with each MCO in their service area
Prior Authorization: Required for all ABA services; updated April 1, 2025 to simplify 90-day extension process
Provider Shortages: Documented by Autism Society of Texas; many providers decline Medicaid due to low rates; families face extended waitlists
Data Transparency: HHSC does not publicly report number of children receiving Medicaid ABA, waitlist lengths, or spending per client by MCO
89th Legislature (2025): Autism Society sought $70M/yr additional funding + data reporting + advisory committee; ECI received $18M increase; ABA-specific rate increase not enacted
HB 564 (89th Leg.): Introduced March 2025 re: health benefit plan coverage for ASD; referred to Insurance Committee; did not advance
Children’s Autism Program: Separate HHSC program; focused ABA limited to 180 hrs/12 months and 720 hrs lifetime; not the same as the Medicaid ABA benefit
Largest TX-Based Providers: Action Behavior Centers (HQ: Austin); Behavioral Innovations (HQ: Addison, 63+ TX clinics); BlueSprig Pediatrics (launched Houston, KKR-backed)
Federal Context: One Big Beautiful Bill Act: $900B+ Medicaid cuts over 10 years; will increase pressure on Texas’s $82.3B Medicaid budget
Key Advocacy Orgs: Autism Society of Texas; TxABA Public Policy Group; Autism Speaks; Disability Rights Texas; The Arc of Texas
SOURCES & REFERENCES
State Agency: Texas Health and Human Services Commission (HHSC); Texas Medicaid & Healthcare Partnership (TMHP)
Legislative Sources: HB 1919 (2007); SB 1484 (2013); SB 589 (licensure); HB 1 Rider 32 (2019); HB 564 (2025); SB 1 (89th Leg. budget)
Advocacy: Autism Society of Texas (texasautismsociety.org); TxABA Public Policy Group
Rate Data: HHSC Provider Finance Department rate tables; TMHP fee schedules; November 2023 and 2024 rate hearings
Industry Sources: Behavioral Health Business; ABA Matrix; Trilliant Health (Dec. 2025)
Federal Context: CMS Informational Bulletin CIB-07-07-14 (July 2014); One Big Beautiful Bill Act (2025)
Session Recap: Texans Care for Children (June 2025); TCDD Disability Policy Academy (June 2025)
Published: BreakingNewsABA.com — March 2026