A Half-Billion-Dollar Line Item
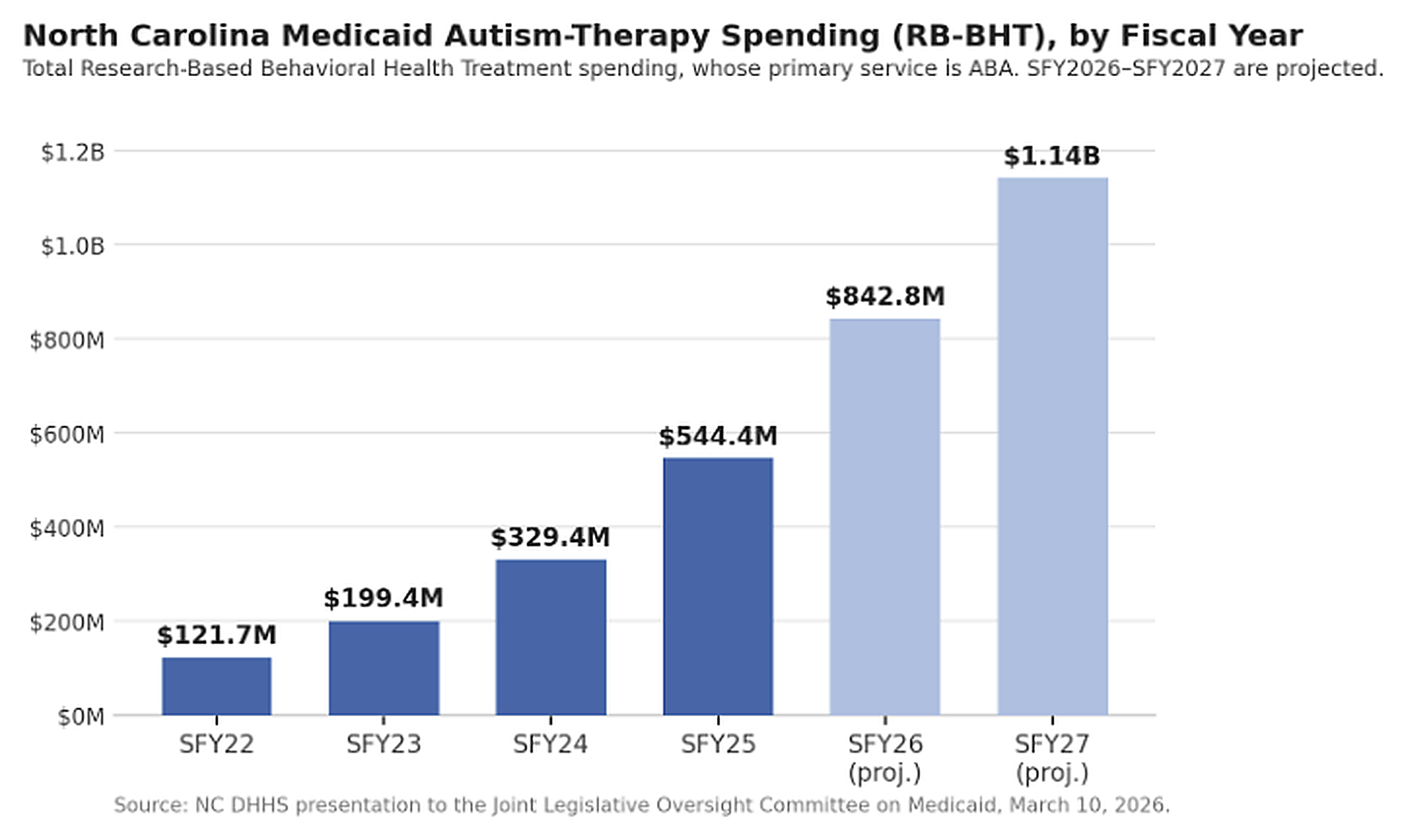
RALEIGH, NORTH CAROLINA – In fiscal year 2022, North Carolina’s Medicaid program spent about $121.7 million on the Medicaid benefit that funds autism behavioral therapy, the bulk of it applied behavior analysis. By fiscal 2025 that spending had reached $544.4 million, and the Department of Health and Human Services projects it will surpass $1.1 billion by 2027. By any measure, that is one of the steepest spending curves in the Medicaid program, and it has put a therapy that many families credit with real progress for their children at the center of a fight over what the state can afford.
The figures DHHS presented to the General Assembly on March 10 trace a near-vertical climb. Total spending on Research-Based Behavioral Health Treatment, the Medicaid benefit suite whose primary service is ABA, rose from $121.7 million in fiscal 2022 to $199.4 million in 2023, $329.4 million in 2024, and $544.4 million in 2025, with projections of $842.8 million in 2026 and $1.14 billion in 2027. ABA accounts for the overwhelming majority of that spending; a North Carolina Health News analysis put ABA outlays specifically at about $505 million in 2025. Over the same window the number of Medicaid members receiving the services grew from 3,844 to 13,447, and children ages one to six absorb roughly 70 percent of the dollars. North Carolina is not alone: DHHS noted that national Medicaid ABA spending grew nearly 300 percent between 2019 and 2024, with reported large increases in Indiana and Nebraska.
How much of the rest is legitimate access expansion and how much is something else is precisely the question North Carolina is now trying to answer. The stakes reach well beyond Raleigh. North Carolina is one of the larger Medicaid ABA markets in the Southeast, and the choices it makes about audits, reimbursement, and utilization controls will be studied closely by other states watching their own spending curves bend upward.
The Auditor’s Alarm
State Auditor Dave Boliek has opened a large-scale review of ABA billing in the Medicaid program. By his office’s accounting, ABA billings, the amounts providers submit, grew to more than $660 million in 2025. The gap between that billed figure and the $505 million the state actually paid reflects the difference between what is submitted and what clears.
Boliek has framed the trajectory as a flashing warning light rather than proof of wrongdoing. His office has said it is examining potential improper payments, lax oversight, and everything in between, and that it is working with other state auditors and federal partners. Among the specific concerns he has raised publicly are billing patterns that suggest weak controls, including instances in which multiple clinicians appear to bill for the same child during overlapping periods, which he attributes in part to gaps in the way the state wrote its rules. Some questionable billing, he has suggested, may be permissible precisely because oversight has been loose. A New York Times investigation published in late May, focused heavily on a large North Carolina provider, amplified the same questions on a national stage.
Improper Documentation or Expanded Access to ABA?
The honest answer is that both explanations can be true at once, and untangling them is the work the audit is meant to do. On the demand side, the growth is not hard to explain in broad strokes. Federal law requires state Medicaid programs to cover medically necessary autism services for children under 21 through the Early and Periodic Screening, Diagnostic and Treatment benefit, and North Carolina built out ABA coverage over the past decade. Autism diagnoses have risen sharply nationwide, screening has improved, and the state extended research-based behavioral treatment to beneficiaries over 21 in 2021. The number of children served more than tripled over three years, which does real work in explaining the totals.
Against that, the auditor’s point is one of proportion. A spending line that multiplies by several hundred percent in three years outruns any plausible increase in the underlying prevalence of autism, which has risen but not at that slope. That mismatch is what invites scrutiny of the supply side: how hours are authorized, how time in a clinic is billed, whether assessments and documentation support the volume, and whether the fee-for-service structure rewards more billed hours regardless of clinical need. None of that is unique to North Carolina. Federal audits in other states have found documentation gaps, uncredentialed staff, and billing for time that is not clearly therapy.
A Few Big Players
The billing is concentrated. An analysis by North Carolina Health News found that of the more than 200 ABA providers in the state’s Medicaid program, 80 received at least $1 million in 2025, and a smaller group captured a disproportionate share. Compleat Kidz, a North Carolina-based chain, collected $51.14 million in Medicaid ABA reimbursement in 2025, and by the New York Times’ accounting had drawn roughly $130 million from the program since 2019, with more than 80 percent of its patients covered by Medicaid. That concentration is the thread connecting the spending story to the business of ABA.

Much of the recent expansion has been financed by private capital. The model that draws scrutiny is recognizable across the industry: long clinic days, high billed hours, and recruitment strategies built to capture market share in a payer that reimburses reliably. Providers counter that demand is real, waitlists are long, and that high billings reflect children who would otherwise go without care. Both descriptions can fit the same clinic.
The same numbers read as potential overbilling to an auditor and as a long-underserved population finally getting care to a provider. North Carolina is now deciding which story governs its rules.
What Comes Next for Providers
The policy response is already taking shape, and it runs along three tracks. DHHS Secretary Devdutta Sangvai has proposed a sweeping revision of Clinical Coverage Policy 8F, the section of state Medicaid rules that governs ABA. The draft, released for public comment on May 15 with comments open through June 14 before the state submits it to the federal Centers for Medicare and Medicaid Services for approval, would tighten oversight of providers, restrict the use of telehealth, and impose new accountability standards on how the therapy is delivered and documented. For providers that built telehealth-heavy or high-utilization models, those changes would land directly on the revenue line.
The second track is reimbursement, and here providers have already won a round. When the state moved to cut ABA rates, families challenged the action in court, and Superior Court Judge Clayton Somers sided with them, noting that DHHS by its own estimates had enough funding to operate through the spring, which made the targeted cuts difficult to justify. The reprieve is unlikely to be permanent. The third track is legislative: the General Assembly reached a Medicaid deal in late April that includes limits and conditions specific to ABA, with implementation phased into late 2026 and 2027. Providers warned that aggressive cuts would have consequences for access. The chief executive of Compleat Kidz testified that a proposed cut would double the existing six-month wait at his Rocky Mount clinic and force the elimination of roughly 100 jobs.
For operators across the state, the practical implications are immediate. Documentation standards, authorization practices, telehealth exposure, and the share of revenue tied to Medicaid all become risk factors to manage rather than assumptions to build on. For investors and acquirers, a market facing simultaneous audit risk, rate pressure, and a rules rewrite is a harder one to underwrite, and valuations that assumed continued open-ended growth will be reconsidered.
A Bellwether for the Southeast
What happens in North Carolina will not stay there. The pattern it is living through, explosive Medicaid-funded growth followed by an audit, a utilization crackdown, and reimbursement pressure, has already played out in states such as Colorado and Minnesota, and the federal government has been auditing state ABA programs in a coordinated wave. North Carolina is large enough, and far enough along, that its choices on telehealth limits, accountability standards, and rate-setting could become a template for other states.
The hard part is the part that does not resolve cleanly. The same dollars that look like a fraud risk from the auditor’s chair look like overdue access from a parent whose child waited months for a slot. Tightening oversight without choking off a population that only recently gained covered care is a genuinely difficult balance. The providers, families, and investors with a stake in the answer will be reading North Carolina’s next moves closely. The audit will eventually report. The rules will change. The spending curve, for now, is still pointing up.
AT A GLANCE
| Spending (2025): | Total RB-BHT (autism therapy) spending reached $544.4 million in fiscal 2025; ABA specifically ~$505 million |
| Projection: | ~$842.8 million in FY2026; ~$1.14 billion in FY2027 (DHHS projections) |
| Trajectory: | $121.7M (FY2022) → $329.4M (FY2024) → $544.4M (FY2025), +347%; projected $842.8M (FY2026), $1.14B (FY2027) |
| Auditor figure: | State Auditor Dave Boliek: ABA billings rose from ~$6 million (2021) to ~$660 million (2025), ~11,000% |
| Children served: | 13,447 people, most of them children, received Medicaid-funded ABA in NC in 2025 |
| Provider concentration: | 80 of 200+ NC Medicaid ABA providers each received $1M+ in 2025; Compleat Kidz collected $51.14M |
| Demand drivers: | EPSDT mandate, rising diagnoses, more children served (3,844 to 13,447), expanded coverage, telehealth |
| Oversight concerns: | Possible duplicate billing, weak DHHS rulemaking, fee-for-service incentives; PE expansion (PESP) |
| Rules: | Proposed Clinical Coverage Policy 8F revisions: tighter oversight, telehealth limits, new accountability |
| Timeline: | Policy 8F draft released May 15, 2026; public comment through June 14; then CMS approval |
| Rate cut: | Attempted ABA rate cut blocked; Judge Clayton Somers sided with families |
| Why it matters: | NC is a Southeast bellwether; outcome could shape audits, rates, telehealth, hiring, and M&A regionally |
SOURCES & REFERENCES
| 1. | North Carolina Health News (Jaymie Baxley). “NC moves to rein in soaring autism therapy costs.” April 27, 2026. https://www.northcarolinahealthnews.org/2026/04/27/autism-therapy-costs/ |
| 2. | Carolina Journal. “NC lawmakers probe surge in autism therapy costs” (March 10 legislative oversight hearing). March 2026. https://www.carolinajournal.com/nc-lawmakers-probe-surge-in-autism-therapy-costs/ |
| 3. | CBS 17 / WNCN. “Autism therapy billing through Medicaid jumped 11,000% in 4 years, prompting a state audit” (Boliek; $6M to $660M). May 15, 2026. https://www.cbs17.com/news/capitol-report/autism-therapy-billing-through-medicaid-jumped-11000-in-4-years-prompting-a-state-audit/ |
| 4. | Fox News. “Medicaid fraud fears grow amid massive billing spike” (Boliek; oversight and fraud concerns; FY2026 and FY2027 projections). May 9, 2026. https://www.foxnews.com/politics/medicaid-fraud-fears-grow-amid-massive-red-state-billing-spike-sector-also-plagued-minnesota- |
| 5. | Carolina Journal. “Autism therapy scrutiny grows after NYT report on NC clinics” (Compleat Kidz; ~$130M since 2019; >80% Medicaid). May 2026. https://www.carolinajournal.com/autism-therapy-scrutiny-grows-after-nyt-report-on-nc-clinics/ |
| 6. | Private Equity Stakeholder Project. “North Carolina moves to rein in autism therapy costs” (PE expansion in ABA). May 6, 2026. https://pestakeholder.org/media_coverage/north-carolina-moves-to-rein-in-autism-therapy-costs/ |
| 7. | Autism Society of North Carolina. “Why ABA Treatment Is in the News in North Carolina” (Policy 8F draft May 15; comment through June 14; CMS). May 19, 2026. https://www.autismsociety-nc.org/policy-legislative-update-may-19-2026-why-aba-treatment-is-in-the-news-in-north-carolina/ |
| 8. | Carolina Journal. “NC House, Senate reach deal on Medicaid funding, oversight reforms” (ABA guardrails; passed 112–3 / 45–3). April 28, 2026. https://www.carolinajournal.com/nc-house-senate-reach-deal-on-medicaid-funding-oversight-reforms/ |
| 9. | NC Medicaid / DHHS. “Clinical Coverage Policy 8F: Research-Based Behavioral Health Treatment.” https://medicaid.ncdhhs.gov/providers/program-specific-clinical-coverage-policies |
| 10. | Disability Rights NC. “Autism-Related Services in NC” (EPSDT coverage; RB-BHT for 21+ effective July 1, 2021). Accessed June 2026. https://disabilityrightsnc.org/resources/autism-related-services-in-nc/ |
| 11. | The Center Square. “North Carolina auditor will probe Medicaid spending for autism therapy” (Cato analysis; $347M to $2.2B national). April 13, 2026. https://www.thecentersquare.com/north_carolina/article_23fbe841-9f5e-4ca1-a219-6e27b48551c3.html |
| 12. | NC DHHS (Sec. Dev Sangvai; Interim Dep. Sec. Melanie Bush). “Update on Autism Benefits,” presentation to the Joint Legislative Oversight Committee on Medicaid. March 10, 2026. (RB-BHT spending $121.7M FY2022 to $544.4M FY2025; 347%; 3,844 to 13,447 members.) https://www.northcarolinahealthnews.org/wp-content/uploads/2026/04/NCGA_Item-5a-DHHS-Medicaid-Autism-Benefits_03.10.2026.pdf |