INDIANAPOLIS, IN— When Indiana’s Medicaid program began covering applied behavior analysis therapy in 2015, the annual cost was manageable: roughly $17 million across a small and growing patient population. No one in state government treated the program’s structure as urgent. Providers were reimbursed at a fixed percentage of whatever they billed. There were no accreditation requirements to operate. There was no dedicated program office to monitor quality or utilization. There was no cap on how many providers could enter the market or how many hours they could bill.
By 2023, the annual cost had reached $611 million. A federal audit of just two years of claims — 2019 and 2020 — found at least $56.6 million in improper Medicaid payments and an additional $76.7 million in potentially improper ones. Indiana was the first of nine states the U.S. Department of Health and Human Services Office of Inspector General planned to audit. Without reform, state projections showed the program reaching $825 million annually by 2029. Indiana had a problem. It also, finally, had a plan to address it.
“When Medicaid coverage for ABA therapy began in Indiana, the program was small and costs were manageable. But with little oversight, spending skyrocketed to unsustainable levels.”
— Eric Miller, Deputy Secretary, Indiana FSSA
How $17 Million Became $611 Million
INDIANA ABA MEDICAID SPENDING — TIMELINE
2015–2017 — Coverage begins. Annual spend ~$17M. No oversight urgency.
2017–2019 — Costs explode from $14.4M to $120M — an 8× increase in two years.
2019–2020 — HHS-OIG audits these two years; finds $56.6M improper + $76.7M potentially improper.
2023 — Annual spending peaks at $611M. Managed care entities raising alarms.
Jan 2024 — Prior Holcomb administration introduces standardized rates (~$68/hr). Smaller providers close or consolidate.
Early 2025 — Holcomb admin proposes retroactive 3-year therapy lifetime cap — would cut off ~50% of enrolled children. Schools not consulted.
Feb 2025 — Gov. Braun rejects the retroactive cap. Signs EO 25-31 creating the ABA Working Group.
May–Sep 2025 — Working Group meets; 4 public sessions; 170+ written submissions; comprehensive review.
Aug 2025 — RBTs required to individually enroll with Indiana Health Coverage Programs (IHCP).
Nov 12, 2025 — Working Group releases ~20 recommendations. FSSA begins implementation phase.
2029 (proj.) — $825M without reform. ~$445M in 2024 after rate standardization.
The shape of Indiana’s problem was not simply that more families were seeking ABA therapy — though that was real, driven by rising autism diagnoses and expanding awareness. The deeper structural issue was the billing model. From 2015 through roughly 2023, Indiana Medicaid reimbursed most ABA services at a flat 40% of whatever a provider charged, regardless of their actual costs. The model created, in the words of Jason McManus, president of Indiana Providers of Effective Autism Treatment (InPEAT), “some very strange incentives for a small portion of the provider network.” Providers who inflated their billed charges received larger reimbursements. Providers with no accreditation requirements, no supervision ratios, and no independent oversight had few checks against doing so.
The federal audit, released in December 2024 by the HHS Office of Inspector General, documented what that environment had produced. Auditors examined 100 sampled enrollee-months and found that 97 out of 100 contained at least one improper payment. Common violations included billing for group services at individual therapy rates, including non-therapeutic activities like meal times and bathroom breaks in billed session hours, insufficient or missing diagnostic evaluations before services began, inadequate documentation, and claims from providers who were not properly credentialed. In the two years audited alone, the OIG recommended Indiana refund $39.4 million to the federal government.
The audit also noted something that should give every state Medicaid director pause: Indiana was the first of nine planned state ABA audits. The OIG had identified the ABA sector nationally as a high-risk area for improper payments, and it was not planning to stop at Indiana.
The Retroactive Cap That Nearly Ended Half the Program Overnight

The first serious attempt to address costs came under Governor Eric Holcomb’s outgoing administration in early 2025. FSSA drafted a State Plan Amendment proposing to cap ABA therapy at three years of comprehensive services per child. The cap was not proposed prospectively — it was retroactive. Children who had already been receiving therapy for three years would have had their services terminated by April 1, 2025. By the state’s own estimate, approximately half of the roughly 8,000 Hoosier children enrolled in Medicaid ABA services would have been cut off immediately. Schools, which were expected to absorb those children, had not been consulted and were not prepared.
“The governor decided this was cruel and unusual punishment, and we weren’t going to do that.”
— Mitch Roob, Secretary, Indiana FSSA
When Governor Mike Braun took office in January 2025, he pulled the proposal. His FSSA secretary, Mitch Roob, called the retroactive cap what it was. A second State Plan Amendment was filed — this one applying prospectively and with a July 1 effective date — but it too was eventually scrapped as the Working Group process got underway. The episode illustrated a tension that would define Indiana’s entire reform effort: the pressure to cut costs quickly was real, the fiscal exposure was significant, but a solution that harmed the children the program was designed to serve was, politically and morally, not viable.
The Market Shock of 2024: Standardized Rates and Consolidation
The Holcomb administration did implement one significant change before leaving office: the introduction of standardized reimbursement rates in January 2024, replacing the open-ended percentage-of-billed-charges model. The new rate for RBT-delivered individual ABA therapy settled at approximately $68 per hour — placing Indiana in the top third of states nationally, but representing a significant reduction from what some providers had been billing and collecting under the prior system.
The effect on the provider market was immediate and uneven. “That did have an impact on the provider community,” McManus told Stateline. “You had a lot of folks, smaller shops, who ended up closing their doors or consolidating with other organizations. So that was disruptive.” The providers most affected were those who had either knowingly built business models around inflated billing, or smaller ethical providers operating on thin margins who could not absorb the reduction. Despite the disruption, total spending still declined only modestly — from $611 million in 2023 to $445 million in 2024 — because utilization continued to increase. The number of ABA therapy locations in Indiana grew 25% between just 2023 and 2025, reaching more than 320 sites, all of which could bill Medicaid without any accreditation requirement.
The Working Group: 21 People, 170 Submissions, and Five Pillars

Governor Braun’s Executive Order 25-31, signed February 19, 2025, established the ABA Working Group under the direction of FSSA and the Indiana Department of Education. The group’s 21 members included state agency leaders, clinicians, legislators, ABA therapy providers, educators, parents, and disability advocates. Its mandate was explicit: find cost-containment strategies that minimize the negative impact on Medicaid enrollees and their families. The group met regularly from May through September 2025, held four in-person listening sessions and one virtual session, heard from nearly 60 Hoosiers, and received more than 170 written submissions.
The final report, released November 12, 2025, contained approximately 20 recommendations organized around five interdependent pillars. FSSA framed the announcement pointedly: “This is Indiana choosing thoughtful reform over arbitrary cuts.”
The Five Pillars of Indiana’s ABA Reform
- Flexible Service Limits A lifetime allocation of up to 4,000 hours of comprehensive ABA per child, followed by ongoing targeted (lower-intensity) therapy. Replaces the blunt retroactive three-year cap. FSSA’s own data found no observable decline in average weekly hours among enrollees after three years of care.
- Caregiver Involvement Requirement Mandate active caregiver participation to reinforce ABA strategies across daily routines — extending therapeutic gains beyond clinic or session hours.
- Federal EPSDT Compliance Explicitly tie the ABA benefit to the Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) federal Medicaid standard, ensuring both floor coverage protections and clearer eligibility and documentation requirements.
- Provider Quality & Oversight Overhaul Require accreditation of all ABA therapy centers (via the Autism Commission on Quality or an approved vendor). Temporary moratorium on new provider sites, with incentives for expansion into underserved rural counties. Mandatory BCBA-to-RBT supervision ratios. RBT individual enrollment with IHCP already implemented August 2025.
- Sustainable Rate & Payer Structure Adjust RBT individual therapy rates as necessary to stay within FSSA’s appropriated budget. Rate modifiers to incentivize group therapy. Quality incentive payments tied to measurable outcomes. Strengthen third-party liability tracking so commercial insurers pay their share above Medicaid rates.
What’s Already in Place — and What Comes Next
The Working Group’s recommendations were not the state’s first move. Standardized rates had been in place since January 2024. Since August 2025, all registered behavior technicians have been required to individually enroll with the Indiana Health Coverage Programs (IHCP) and submit documentation to each managed care entity — enabling background checks, fingerprinting, credential verification, and direct oversight of supervision ratios for the first time. FSSA also initiated a program integrity review of all Medicaid ABA claims paid from 2022 through 2025; when complete, providers with improper payments will be required to refund overpayments and complete compliance training.
The accreditation requirement is the reform with the longest runway. The Working Group’s report indicated preliminary conversations had begun with the Autism Commission on Quality, but implementing accreditation across Indiana’s 320-plus provider locations would take roughly a year. The temporary moratorium on new provider sites, if implemented, would freeze that number while accreditation infrastructure is built out. The commercial payer TPL enforcement piece, if effective, could shift a meaningful portion of ABA costs off the Medicaid ledger entirely.
How Providers and Families Are Reading the Reform
Provider reaction to Indiana’s reform effort has been more nuanced than the blunt opposition that Nebraska’s cuts generated. Indiana’s approach involves a consultative process, prospective implementation, and explicit commitments to protect currently enrolled children. The retroactive cap was rejected before it could cause harm. That sequencing bought the state a degree of credibility with providers and families that Nebraska did not establish.
Not every voice is satisfied. Susan Crowell, executive director of My Autism Ally and a Working Group member, praised several recommendations — mandatory caregiver involvement, BCBA-to-RBT supervision ratios, removal of virtual RBT oversight — while expressing pointed frustration with the state’s handling of those who exploited the billing loopholes that created the problem. “The ABA therapy providers who exploited the loophole that Indiana Medicaid created are better positioned financially to survive these cuts than the ethical providers that were unaware of or did not exploit the loophole,” she wrote publicly. “This puts many of our Hoosier-owned ABA therapy providers at a disadvantage.”
“This is Indiana choosing thoughtful reform over arbitrary cuts.”
— Mitch Roob, Secretary, Indiana FSSA, November 12, 2025
Indiana’s Audit Was First of Nine. The Field Is Watching.
Indiana’s situation carries national significance. The HHS-OIG’s December 2024 report was explicit: Indiana was the first of nine planned state Medicaid ABA audits. In July 2025, Wisconsin became the second, with the OIG finding at least $18.5 million in improper ABA payments. The same documentation and credentialing failures that defined Indiana’s audit — billing group services as individual therapy, inadequate session notes, improperly credentialed providers, missing diagnostic evaluations — are patterns the OIG has identified as systemic across states that built ABA coverage quickly, without the oversight infrastructure to match.
The enforcement environment has also intensified at the state level. Massachusetts’ Attorney General’s Office indicted an ABA provider in June 2025 for allegedly fabricating documentation to support over $1 million in false claims. Kevin Lownds, division chief at Massachusetts’ Medicaid Fraud Control Unit, stated publicly that ABA was an area where fraud warranted criminal charges and that his unit was seeing it regularly. Indiana’s $39.4 million federal refund recommendation, the nine-state audit series, and the working group reforms collectively describe an industry at an inflection point. The ABA market was built on coverage mandates, federal funding, and high rates. The oversight infrastructure that should have accompanied that growth lagged years behind. Indiana’s reform effort is an attempt to build that infrastructure retroactively, without destroying access for the 8,000 Hoosier children whose care now depends on its survival.[divider line_type=”Full Width Line” line_thickness=”1″ divider_color=”default”]Key Facts at a Glance
Spending 2017: $14.4M (fee-for-service)
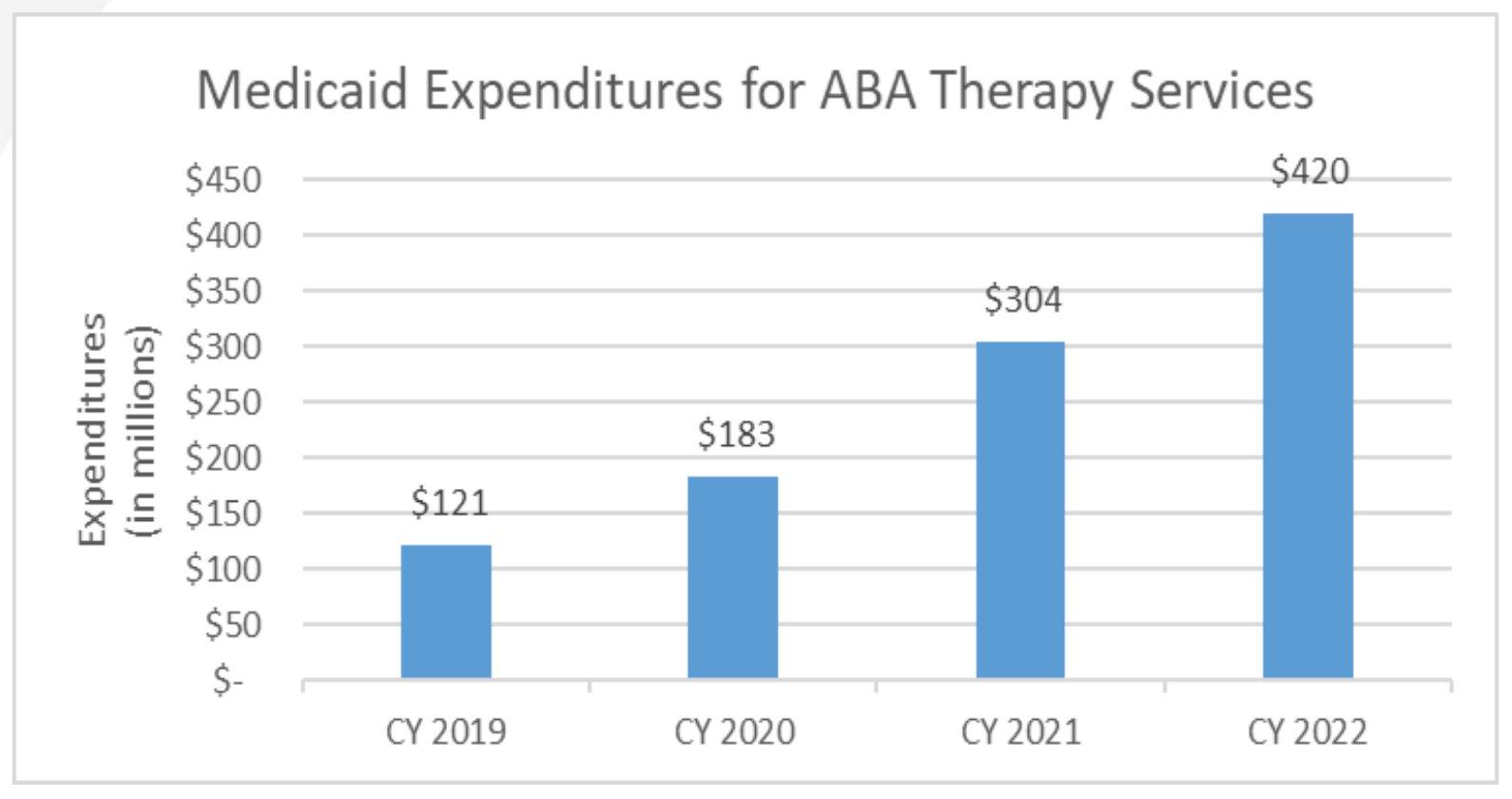
Spending 2019: $121M
Spending 2020: $183M
Spending 2021: $304M
Spending 2022: $420M
Spending 2023: $611M — nearly 3,000% increase in 6 years
Spending 2024: $445M (after rate standardization)
Projected 2026: $645M+ without reform
Projected 2029: $825M without reform
Children enrolled: ~8,000 Hoosiers on Medicaid-funded ABA
HHS-OIG audit (2019–2020): $56.6M improper + $76.7M potentially improper = $133M+ in question
Federal refund recommended: $39.4M (federal share)
OIG audit scope: Indiana first of 9 planned state ABA audits nationally
Prior billing model: 40% of billed charges (no ceiling) — removed Jan 2024
Current RBT rate: ~$68/hr (top third nationally; above national avg of $61)
Provider count: 320+ locations; 25% growth 2023–2025
Accreditation requirement: None currently — mandatory requirement recommended
RBT enrollment: Required individually with IHCP since August 2025
Key Voices
Gov. Mike Braun: Signed EO 25-31, Feb 2025 — in.gov
Mitch Roob: Secretary, Indiana FSSA
Eric Miller: Deputy Secretary / Chief of Staff, Indiana FSSA
Jason McManus: President, Indiana Providers of Effective Autism Treatment (InPEAT)
Mariel Fernandez: VP Government Affairs, Council of Autism Service Providers (CASP)
Susan Crowell: Executive Director, My Autism Ally; Working Group member — myautismally.org
Emily Roche: VP Payer Contracting, Bierman Autism Centers
Key Documents & Sources
Working Group Final Report: EO 25-31 ABA Working Group Recommendations — November 12, 2025 — in.gov/fssa
HHS-OIG Audit: December 19, 2024 — oig.hhs.gov
Indiana Capital Chronicle: indianacapitalchronicle.com
Stateline: stateline.org — “Families worry as cost of autism therapy comes under state scrutiny” (Nov. 2025)
STAT News: statnews.com — “Indiana Medicaid audit finds questionable payments” (Dec. 19, 2024)
ABA Reimbursement-Provider Meeting: August 8, 2023 — Indiana FSSA / OIG source data