The calendar tells you everything
Three care management organizations serve Georgia Families Medicaid today. Two of them, Centene’s Peach State and Elevance’s Amerigroup, lost their contract rebids in December 2024. Peach State has already begun terminating provider agreements. Amerigroup’s claims processing has degraded since 2025. Their contracts expire June 30, 2026.
Three new CMOs (Humana, Molina, and UnitedHealthcare) won the rebid. They do not go operational until July 1, 2026. Until then, they cannot credential providers or pay claims.
That leaves CareSource. The sole renewed incumbent. The only fully functioning network in the market. And, by the natural mechanics of a transition, the CMO whose membership is growing as the exiting plans wind down.
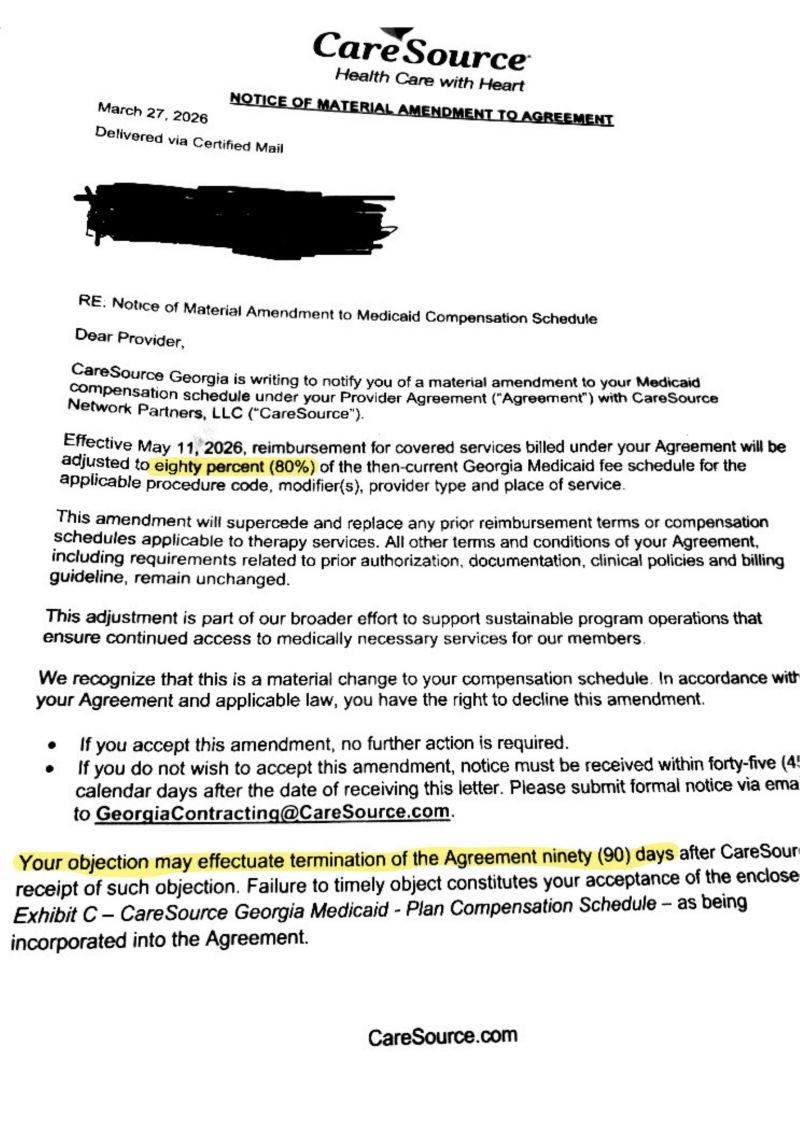
On March 27, 2026, by certified letter, CareSource notified Georgia ABA providers that effective May 11, it was cutting reimbursement by 20% across the board. Forty-five days to object. No actuarial filing. No public process. No press release. Peach State proposed the same 20% cut and paused after provider and family pushback. CareSource didn’t have to.
This was not a rate adjustment. It was leverage exercised in a window the market created and regulators allowed to open.
A CMO is not a rate-setter. Georgia is.
Georgia’s Medicaid program publishes a fee schedule for ABA services, set through the state’s own actuarial work and public rulemaking process. CareSource has unilaterally decided to pay 20% less than that schedule.
ABA for children on Medicaid is not an optional benefit. It is covered under EPSDT, a federal entitlement. The state has an affirmative obligation to ensure access. A CMO operating as a shadow rate-setter, by private letter, on 45 days’ notice, with no actuarial justification, is the state ceding its rate-setting authority by inaction.
Imagine a contractor on a state highway project unilaterally cutting subcontractor pay 20% mid-build because their margins were tight, while the state stayed silent. The road still has to be built. The state still has to pay. The only people absorbing the cut would be the people doing the work. Nobody would call that a market outcome. They’d call it a procurement failure.
ABA Rate cuts cause losses and provider exit
This is the part general-audience commentators get wrong, and it’s worth being precise about.
ABA cost structures are overwhelmingly fixed. BCBA salaries are set by a national labor market that does not care about Georgia’s reimbursement decisions. RBT wages are set by Georgia’s own labor market, where ABA already competes against fast food and retail. Supervision ratios are clinically mandated. Leases, software, billing infrastructure: all fixed.
Most BCBA-owned practices in this country operate on 8–15% margins in a strong year. A 20% rate cut in ABA does not lead to profit compression. It leads to massive provider operating losses and an exodus of providers.
This is the difference between asking a restaurant to lower its menu prices and telling that restaurant its largest delivery partner will now pay 80 cents on the dollar, while ensuring no competing delivery app comes to market for the next nine months. The kitchen either cooks at a loss or closes.
And the CareSource amendment is not even ABA-specific. The letter applies to all services covered under the provider agreement. Multi-disciplinary pediatric clinics (speech, occupational therapy, and ABA under one roof) take the cut across the entire portfolio. One Savannah pediatric therapy clinic owner told local press she will have to discharge all 89 of her CareSource patients across the full service line. CareSource was a third of her caseload.
Who survives this, and who doesn’t
A 20% cut does not hit all providers equally. It hits BCBA-owned independents hardest.
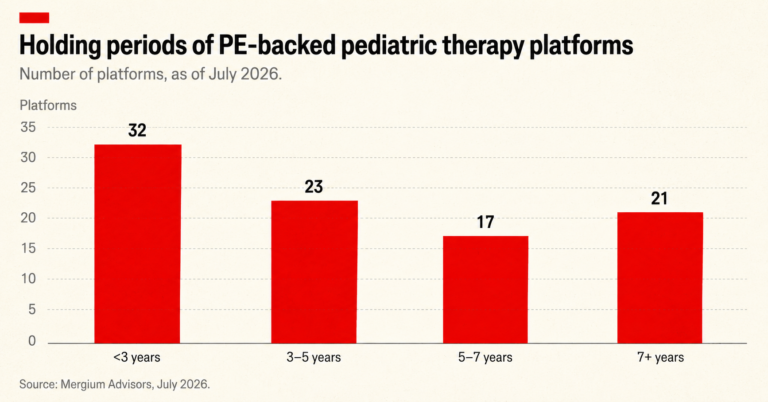
Private-equity-backed multi-state ABA platforms have geographic diversification. Georgia is one market of many. They have access to capital: warchests built explicitly to weather 12 to 18 months of operating losses in a single state. They have centralized back-office cost structures that can absorb fixed-cost erosion the way a single-clinic operator cannot.
The independents (often clinician-owned, the ones embedded in their communities for a decade or more) have none of that.
The predictable second-order effect of a cut like this is accelerated consolidation. Independents close or get acquired at distressed valuations. The same platforms whose productivity-driven, scaled-down clinical models have been criticized by BCBAs for years are the ones positioned to absorb the displaced caseload.
The irony is sharp: a cut justified as “responsible stewardship of taxpayer dollars” produces a market structure in which the operators most aligned with the financial incentives that drive ABA overspending (the high-volume, high-productivity, scale platforms) are the ones that survive.
The damage you cannot undo
Even if Georgia or CareSource reverses course in 12 months, even in six, the damage is structural and largely permanent.
Clinics that close do not reopen because a rate gets restored. BCBAs who leave the state or leave the field do not return because a Medicaid plan publishes a corrected fee schedule. Landlords who watched their ABA tenants default learn that ABA is a credit risk and price the next lease accordingly. Rebuilding ABA infrastructure in Georgia after this kind of contraction will take years.
A two-year-old diagnosed in Thomasville today does not have years to wait. The clinical evidence on early intensive intervention is among the most robust findings in developmental psychology. The developmental window narrows whether or not the rates get restored.
A federal mandate to serve at a loss is not a mandate. It is the policy equivalent of issuing every Georgia child a library card while closing the libraries. EPSDT entitles a Georgia child on Medicaid to medically necessary ABA. If no clinic in driving distance is in-network, the entitlement is theoretical.
A Thomasville ABA clinic founder told local press, in plain terms, that the right therapies are the difference between a child being able to live independently as an adult and living with their parents for the rest of their lives. That is not advocacy rhetoric. It is a clinical consensus.
The clinics most at risk of closure are in rural south Georgia, places where “find another provider” means a four-hour round-trip drive, multiple times a week, that no working parent can sustain. The cost does not disappear. It transfers: to schools, to families, to the adult disability service system, and to Medicaid itself years from now, when the same children need a different and far more expensive level of support.
The rebuttal, answered
The honest steel-man for the cut is real and worth naming. Audits have flagged compliance problems. There are legitimate questions about utilization rigor, prior authorization practice, and whether 30–40 hour weekly regimens are always clinically justified.
Agreed on every count. The response to a utilization problem is utilization management: outcome measurement, tiered rates that reward quality, prior-auth reform, fraud enforcement, audits with teeth. The response to a spending problem is structural payment reform, not a blunt 20% cut imposed by a single CMO on 45 days’ notice.
A flat cut applied to every code, every modifier, every place of service, every provider (regardless of outcomes, complexity, or quality) is the opposite of payment reform. It punishes the high-quality providers exactly as much as the low-quality ones. And the worst actors, the ones with the largest billing operations and the lowest clinical standards, are the ones best-equipped to survive it.
If anyone at CareSource wants to explain how a flat 20% cut produces better outcomes, I’m listening. I’d guess that conversation hasn’t happened. To my reading, the cut isn’t about outcomes. It’s about margin.
To Governor Kemp, Commissioner Burke, and the incoming CMOs
This is the part where rhetoric has to meet action.
To Governor Kemp: Direct DCH to require any CMO rate change affecting a federally mandated EPSDT benefit to be filed with the department, justified actuarially, and subject to a public comment period before taking effect. This is normal regulatory practice in Medicaid agencies across the country. Georgia should not be the exception. A single CMO acting as shadow rate-setter for federally mandated pediatric services, during a regulatory transition, is exactly the failure mode the state is supposed to prevent.
To Commissioner Burke: You spent your career in southwest Georgia rural healthcare. You know what happens to a community when its specialty providers disappear. The clinics most exposed to this cut are in your region. Pause the CareSource amendment for 120 days, through the July CMO transition and into the new network’s operational stabilization. You do not have to litigate whether 20% is the right number. You only have to recognize that no rate change of this magnitude should take effect during a network transition where providers have no alternative payer to migrate to. A 120-day pause costs CareSource nothing it cannot recover. It buys Georgia’s ABA infrastructure the runway it needs to survive into the new contract period intact.
To Humana, Molina, and UnitedHealthcare: You are inheriting a market in July. Tell the providers, in writing, before July 1, what you intend to pay. Commit to honoring the Georgia Medicaid fee schedule. Make it possible for clinic owners to make rational business decisions before they close their doors. You will be far better served inheriting an intact provider network than inheriting one in collapse, scrambling to credential whoever is left.
To my fellow operators: This is not a contract amendment any single practice can negotiate its way out of. CareSource holds the leverage individually and loses it collectively. Organize, file jointly, and make sure the families you serve, and the press that covers them, know exactly what is happening and exactly when. The work you do is too important and too consequential to be marginalized.
What is actually at stake
Georgia spent more than a decade building access to ABA for children who could not advocate for themselves. A single CMO can dismantle that infrastructure in ninety days.
This is a regulatory failure. It is a failure to preserve access to a federally mandated benefit. It is a failure of the commitments this state made to its most vulnerable families: the families with the fewest options, the least political power, and the most to lose. Their children will lose treatment not because the treatment didn’t work, but because the people responsible for protecting their access decided that protecting margin was easier.
A two-year-old in Thomasville does not know what a CMO is. Her parents do not know what EPSDT is. They will only know that the clinic that was going to give their child a chance at independence (at speech, at communication, at a life of her own choosing) closed its doors. And they will be told by everyone who could have prevented it that the timing was unfortunate.
The timing was not unfortunate. The timing was the strategy.
ABA clinics are closing. Children are getting discharged from services. The infrastructure is degrading with each passing day. Every day this amendment stands in force is a day Georgia tells those families that their children’s care is the variable in someone else’s margin equation. That is not who Georgia has been on this issue. And it is not who Georgia has to be on July 1.
AT A GLANCE
| Rate change: | 20% cut from the Georgia Medicaid fee schedule, applied to all covered services under the CareSource provider agreement, effective May 11, 2026 |
| Notice mechanism: | Certified mail dated March 27, 2026; 45-day window to object; no public announcement; no actuarial filing released |
| Provider options: | Accept the cut (silence treated as acceptance) or object and trigger a 90-day termination of the CareSource provider agreement |
| Market context: | CareSource is the sole CMO with a renewed contract; Peach State (Centene) and Amerigroup (Elevance) lost their bids and are winding down |
| Peach State comparison: | Initially proposed the same 20% cut; paused after provider and family pushback |
| Incoming CMOs: | Humana, Molina, and UnitedHealthcare were awarded contracts in December 2024; transition originally targeted July 1, 2026, reportedly delayed to mid-2027 (State Affairs reporting via Autism Providers of Georgia) |
| CareSource statement: | Cut “reflects national trends” and supports “responsible stewardship of taxpayer dollars” (CareSource public statement, May 2026) |
| DCH position: | The Georgia Department of Community Health said it was “not involved” in the rate decision and will increase network adequacy monitoring (Capitol Beat) |
| Federal framework: | ABA for Medicaid-enrolled children is covered under the federal EPSDT entitlement; states have an affirmative obligation to ensure access |
| Central argument: | A CMO unilaterally cutting reimbursement during a regulatory transition, with no actuarial filing or public process, is a governance failure rather than a market outcome |
| Recommended actions: | Commissioner Burke pauses the amendment for 120 days; Governor Kemp directs DCH to require actuarial filing and public comment for any future MCO rate change affecting EPSDT benefits; incoming CMOs publicly commit to honoring the Georgia Medicaid fee schedule before launch |
SOURCES & REFERENCES
| 1. | Breaking News ABA. “CareSource Georgia Unilaterally Slashes ABA Rates 20% Leaving ABA Families and Providers Scrambling.” Published May 20, 2026. https://breakingnewsaba.com/policy/caresource-georgia-unilaterally-slashes-aba-rates-20-leaving-aba-families-and-providers-scrambling |
| 2. | Acuity.news. “Georgia ABA Alert: CareSource Slashing Medicaid Rates by 20%.” Published April 2026. https://acuity.news/regulation/georgia-medicaid-aba-caresource-rate-cut-2026/ |
| 3. | Capitol Beat / Moultrie Observer. “Pending Cuts to Georgia Medicaid Payments Could Affect Children Who Need Therapy.” Published April 25, 2026. https://www.moultrieobserver.com/2026/04/25/pending-cuts-to-georgia-medicaid-payments-could-affect-children-who-need-therapy/ |
| 4. | WTXL Tallahassee. “Medicaid Cuts Threaten to Close South Georgia Autism Therapy Clinics.” Published May 5, 2026. https://www.wtxl.com/news/local-news/in-your-neighborhood/thomas-county/medicaid-cuts-threaten-to-close-south-georgia-autism-therapy-clinics |
| 5. | OPEN MINDS. “CareSource Georgia Cuts Medicaid ABA Rates 20%.” Published May 2026. https://openminds.com/market-intelligence/news/caresource-georgia-cuts-medicaid-aba-rates-20/ |
| 6. | Atlanta Journal-Constitution. “Inside the ‘Big Deal’ Battle for Georgia’s Multibillion-Dollar Medicaid Contract.” Published December 24, 2024. https://www.ajc.com/politics/inside-the-big-deal-battle-for-georgias-multibillion-dollar-medicaid-contract/ZWBDMVJBTJH63PTDE6NPS2JBAY/ |
| 7. | Becker’s Payer Issues. “Georgia to Award 4 Medicaid Contracts.” Published December 5, 2024. https://www.beckerspayer.com/contracting/georgia-to-award-4-medicaid-contracts/ |
| 8. | WABE. “Fight Over Georgia’s Medicaid Contracts Nears the End, as Foster Parents Plead for Reversal.” Published December 15, 2025. https://www.wabe.org/fight-over-georgias-medicaid-contracts-nears-the-end-as-foster-parents-plead-for-reversal/ |
| 9. | Georgia Department of Community Health. “Medicaid Managed Care.” Accessed June 2026. https://dch.georgia.gov/medicaid-managed-care |
| 10. | Centers for Medicare & Medicaid Services. “Early and Periodic Screening, Diagnostic, and Treatment (EPSDT).” https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-treatment/index.html |