132,307 Job Postings and a Moderating Growth Rate
ACROSS THE UNITED STATES — The Behavior Analyst Certification Board, in partnership with the labor market data firm Lightcast, released its latest workforce demand data in early 2026. The headline number: 132,307 job postings for BCBAs and BCBA-Ds in 2025, a 28 percent increase over the prior year. The figure continues the exponential trajectory of BCBA demand that has defined the ABA labor market for the past decade—but the rate of increase moderated significantly from 2024, when job listings grew by 58 percent.
The geographic concentration of demand remains extreme. Five states—California, New Jersey, Texas, Massachusetts, and North Carolina—account for 38 percent of all BCBA job postings, with California alone representing 15 percent of 2025 demand. Very few states saw a reduction in the number of open positions. The data confirm what ABA practice owners and PE sponsors already know: the demand for BCBAs is not cyclical but structural, driven by rising autism prevalence, expanded insurance mandates, and a service model that requires supervisor-level clinicians to design and oversee every treatment plan.
The Lightcast data also revealed a notable divergence in demand by credential level. While BCBA and BCBA-D job postings surged, listings for BCaBAs—board-certified assistant behavior analysts—dropped significantly year over year. The decline suggests that employers are increasingly prioritizing independently licensed supervisor-level clinicians over mid-level practitioners, a trend that compresses the workforce bottleneck further at the BCBA level.
The 132,307 job postings represent the visible demand. The invisible demand—families on waitlists, children aging out of early intervention windows while waiting for services, providers declining new cases due to BCBA capacity constraints—is almost certainly larger.
The National Shortage: Five Times More BCBAs Needed
A January 2026 analysis published by TYGES, a healthcare staffing and recruitment firm, quantified the BCBA shortage with a level of specificity that the industry had lacked. Using BACB certificant data as of October 2025, CDC autism prevalence estimates, and U.S. Census population data, TYGES calculated the gap between the current BCBA workforce and the estimated need.
The numbers are stark. As of October 2025, the BACB reports 71,371 BCBAs and 2,915 BCBA-Ds practicing in the United States—a total of 74,286 supervisor-level clinicians. Using the CDC’s most recent autism prevalence estimate of 3.2 percent among eight-year-olds (approximately 1 in 31) as a rough proxy for the population aged 21 and under, TYGES estimated approximately 2.9 million individuals on the autism spectrum in the target age range. Using a conservative planning benchmark of 8 clients per BCBA, the analysis found that the country would need approximately 362,500 BCBAs—nearly five times the current supply.
The shortfall deepens when accounting for the composition of the existing workforce. Research published in Psychiatric Services found that only approximately 72 percent of BCBAs report autism as their primary area of practice. Applying that ratio to the current workforce yields approximately 53,486 BCBAs focused primarily on autism, leaving an estimated gap of more than 309,000 BCBAs needed just to serve the autism population at benchmark caseload levels—before accounting for I/DD, mental health, education, and other practice areas where BCBAs also work.
The total BACB-certified workforce is larger: 320,699 certificants across all credential levels, including 242,327 RBTs, 4,086 BCaBAs, and the 74,286 BCBAs and BCBA-Ds. But RBTs and BCaBAs cannot independently design or supervise treatment plans, meaning the bottleneck is specifically at the BCBA supervisor level. Adding more RBTs without proportionally adding BCBAs simply increases the ratio of technicians to supervisors, creating supervision burden without expanding treatment capacity.
The math is simple and unforgiving: 74,286 BCBA-level clinicians serving an estimated 2.9 million children and young adults with autism means each BCBA would need to carry a caseload of approximately 39 clients—nearly five times the 8-client planning benchmark that workforce researchers use.

The Geography of Care Deserts
The national shortage obscures an even more severe geographic maldistribution. The TYGES analysis calculated BCBAs per 100,000 residents by state, revealing a dramatic range. Massachusetts leads the nation at 55.1 BCBAs per 100,000 residents. New Hampshire (45.6), Connecticut (41.9), and New Jersey (39.2) follow. At the other end, states like Mississippi, Montana, Wyoming, and others in the rural South and Mountain West have BCBA density figures well below 15 per 100,000—and many individual counties within those states have zero BCBAs.
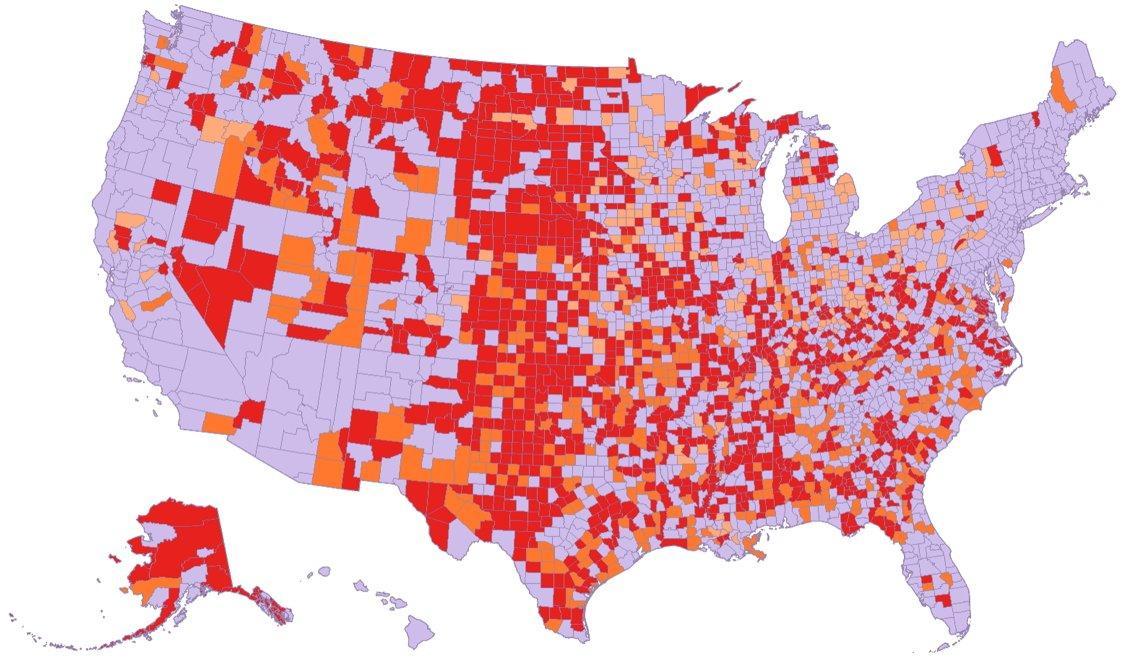
The county-level data is where the care desert reality becomes most concrete. More than half of all U.S. counties have no Board Certified Behavior Analyst practicing within their borders. For families in these counties, the autism diagnosis that was supposed to unlock access to evidence-based treatment instead initiates a search for services that may require driving hours each way, relocating, or going without. Children in rural areas with a current diagnostic status of ASD are more likely than their urban counterparts to report significant difficulties and delays due to lack of available services—35 percent in rural areas compared to 23 percent in urban areas, a 12-percentage-point disparity that represents thousands of children who cannot access timely interventions during critical developmental windows.
The factors driving geographic maldistribution are structural rather than accidental. BCBAs and RBTs concentrate in urban markets where higher caseloads, better compensation packages, and more career advancement opportunities are available. Rural practices often cannot match urban salary offerings, and the professional isolation of rural practice—limited opportunities for collaboration, continuing education, and specialization—makes retention even more difficult than in metropolitan areas. The BACB’s certificant data reflects this reality: a handful of high-density states absorb a disproportionate share of the national workforce, while vast geographic swaths of the country operate as clinical deserts.
Telehealth as a Partial Bridge
Telehealth represents the most frequently cited solution for bridging rural ABA access gaps, and the COVID-19 pandemic demonstrated both the feasibility and the limitations of remote service delivery. Several telehealth models have emerged for delivering ABA services: direct teletherapy, in which BCBAs conduct sessions via video conferencing; parent training and coaching, in which BCBAs train caregivers to implement strategies during daily routines; and hybrid models that combine periodic in-person visits with regular telehealth supervision—maximizing clinical effectiveness while reducing the geographic barrier.
The evidence base for telehealth ABA is growing. Research has shown that telehealth can be effective for parent training, with parents achieving high fidelity in implementing behavior-analytic strategies when coached remotely. Studies have demonstrated over 90 percent reduction in challenging behaviors among children with autism receiving telehealth-delivered interventions. Total costs for home telehealth models have been found to be significantly lower than traditional in-home therapy, making the economic case alongside the access case.
But telehealth ABA has structural limitations that prevent it from fully substituting for in-person services. ABA therapy is fundamentally a hands-on intervention—particularly for younger children, those with more significant support needs, and those working on motor, sensory, or daily living skills that require physical prompting and environmental manipulation. The BCBA can supervise and coach remotely, but the person delivering the hands-on intervention in the room still needs to be a trained technician. In rural areas where the RBT workforce is also thin, telehealth supervision without a local RBT to implement the plan creates a model that works for parent coaching but not for intensive direct therapy.
Infrastructure barriers compound the clinical limitations. In rural areas, 28 percent of people lack access to high-speed broadband internet. On Tribal lands, 24 percent lack broadband access. Small devices like smartphones are not recommended for telehealth ABA delivery because they show a limited view of the client, caregiver, and environment. Laptops and desktop computers are preferred, but not all families in underserved areas have access to appropriate technology. The digital divide and the ABA access divide overlap almost perfectly—the communities with the fewest BCBAs are often the same communities with the least reliable internet.
Telehealth can extend the reach of BCBAs, but it cannot replace the hands-on RBT workforce that ABA therapy requires. In rural counties with zero BCBAs and few RBTs, the access problem is not a technology problem—it is a workforce distribution problem that technology alone cannot solve.
Policy Levers and the Path Forward
Addressing the BCBA shortage and the geographic maldistribution of the ABA workforce will require interventions at multiple levels. At the federal level, loan forgiveness programs for BCBAs who commit to practicing in underserved areas—modeled on the National Health Service Corps framework used for physicians—could incentivize geographic redistribution of the workforce. Rural residency programs and specialized training tracks focused on rural service delivery could build a pipeline of clinicians prepared for non-urban practice from the start.
At the state level, reimbursement parity for telehealth services—ensuring that remote ABA sessions receive equivalent compensation to in-person care—is critical for making telehealth models financially sustainable for providers. States that have achieved reimbursement parity have seen faster adoption of telehealth ABA, while states without parity create a disincentive for providers to invest in the infrastructure needed to deliver remote services at scale.
At the industry level, the expansion of university ABA programs—both master’s and bachelor’s level—continues to grow the pipeline of future BCBAs and BCaBAs. The BACB has reported steady year-over-year increases in exam applications. If the current trajectory holds, the BCBA workforce could exceed 100,000 certificants within a few years. But even at that pace, the growth will not close a gap that requires five times the current supply. And without targeted interventions to address geographic distribution, growing the overall number of BCBAs may simply concentrate more clinicians in the states and metropolitan areas that already have the highest density.
The ABA industry’s workforce crisis is not a temporary disruption. It is a structural feature of a field that has grown faster than its training pipeline, that concentrates its workforce in high-density urban markets, and that relies on a service model requiring a ratio of supervisor-level clinicians to clients that the current workforce cannot support. The 132,307 job postings in 2025 quantify the demand. The county-level data quantify the access gap. The question for policymakers, practice owners, and the certification boards that govern the profession is whether the interventions will match the scale of the problem—or whether the care deserts will continue to expand even as the national workforce grows.
AT A GLANCE
| BCBA/BCBA-D job postings (2025): | 132,307 (28% increase YOY; BACB/Lightcast) |
| Prior year growth rate: | 58% increase in 2024 |
| Top 5 states (% of demand): | CA, NJ, TX, MA, NC (38% combined; CA alone = 15%) |
| BCBAs in U.S. (Oct 2025): | 71,371 BCBAs + 2,915 BCBA-Ds = 74,286 supervisor-level |
| Total BACB certificants: | 320,699 (including 242,327 RBTs, 4,086 BCaBAs) |
| Estimated need: | ~362,500 BCBAs (5x current supply; TYGES analysis) |
| Autism prevalence (CDC): | 1 in 31 among 8-year-olds (3.2%; 2022 ADDM data) |
| Counties with zero BCBAs: | More than half of all U.S. counties |
| Rural vs. urban access gap: | 35% rural vs. 23% urban report significant service delays |
| Highest BCBA density: | Massachusetts (55.1 per 100K) |
| Rural broadband gap: | 28% of rural residents lack high-speed internet |
| BCBAs in autism (est.): | ~53,486 (72% of BCBAs report autism as primary practice area) |
SOURCES & REFERENCES
| 1. | Behavioral Health Business. “Demand for BCBAs Continues Exponential Growth Despite Slight Slowdown.” February 17, 2026. bhbusiness.com. |
| 2. | BACB / Lightcast. “2026 Demand Data.” bacb.com. PDF. January 2026. |
| 3. | TYGES. “Applied Behavioral Analysis (ABA) Care Deserts in the U.S.: A State-by-State Look at BCBA Shortages.” January 16, 2026. tyges.com. |
| 4. | BACB. “BACB Certificant Data.” bacb.com. (74,286 BCBAs/BCBA-Ds; 242,327 RBTs; 320,699 total as of October 2025.) |
| 5. | CDC. “Autism Spectrum Disorder Data and Research.” cdc.gov. (1 in 31 among 8-year-olds, 2022 ADDM Network.) |
| 6. | Links ABA. “ABA in Rural Areas: Access, Telehealth, and Equity.” June 2025. linksaba.com. |
| 7. | Links ABA. “ABA in Underserved Communities: Bridging the Gap.” August 2025. linksaba.com. |
| 8. | Dounavi, K., et al. “Telehealth as a Model for Providing Behaviour Analytic Interventions to Individuals with Autism Spectrum Disorder: A Systematic Review.” Journal of Autism and Developmental Disorders. 2019;49:582–616. |
| 9. | Psychiatry Online. “Geographic Distribution of the ABA Workforce.” Psychiatric Services. 2020. (72% of BCBAs practice primarily in autism.) |
| 10. | U.S. Census Bureau. “Population Estimates by Single Year of Age: 2024.” census.gov. |
| 11. | ATCC. “RBT in 2026: Salary, Demand, and BACB Training Requirements.” January 2026. atcconline.com. (232,792 RBT certificants; 9.6 children with ASD per RBT.) |