The 49th State, and Already Cutting
ALBANY, NEW YORK – most states that cut ABA Medicaid reimbursement rates do so from a position of excess. Nebraska slashed its 97153 rate by 48 percent in August 2025 after the state had paid the highest Medicaid ABA rates in the nation for years. Florida entered its restructuring with a $2.6 billion annual ABA Medicaid spend. New York is doing something different: it is cutting a program that has barely had time to function. New York launched ABA coverage under its Medicaid fee-for-service program on August 1, 2021 — making it the 49th state to implement the benefit. Due to implementation delays, enrolled Licensed Behavior Analysts did not begin using the program at meaningful scale until 2023. The benefit still has not been fully implemented in its authorized form.
Now the state is retreating. As authorized by the NYS Enacted Budget for FY 2025–2026, the New York State Department of Health reduced the fee-for-service rate for CPT code 97153 — adaptive behavior treatment by an unlicensed individual or technician, the code that accounts for the largest volume of ABA hours nationally — to $16.85 per 15-minute unit, effective October 1, 2025 for fee-for-service and December 1, 2025 for Medicaid Managed Care enrollees. A second reduction, to $14.45 per unit, is scheduled for April 1, 2026. The reductions were disclosed in the New York State Medicaid Update for August 2025, Volume 41, Number 8.
To understand what $14.45 per unit means in context: Nebraska’s pre-cut rate of $36.11 was the highest in the nation per the Council of Autism Service Providers’ 50-State Applied Behavior Analysis Medicaid Benefit Comparison published July 2024. New York at $14.45 would be $57.80 per hour — a figure lower than the national average and substantially below the rates paid in high-demand states like Massachusetts, Maryland, and Colorado, all of which have no annual dollar cap and no age restriction on their commercial insurance mandates. For providers considering whether to enter, remain in, or expand within New York’s Medicaid market, the two-step reduction and its trajectory signal a state that is treating its newest benefit as a cost problem rather than a care investment.
The New York State Association for Behavior Analysis opposed the cuts in testimony submitted to the Legislature, characterizing the $9.6 million reduction for FY 2025–26 and the $19 million reduction for FY 2026–27 as harmful to populations that have waited years for access. NYSABA noted that the full ABA Medicaid benefit authorized by the Legislature — which is intended to cover not only children with ASD but also children and adults with mental health diagnoses, including those in foster care and juvenile justice programs — has not yet been implemented. “The proposed cut feels like a reaction to this population finally being allowed to access the medical care they have been prescribed to receive,” the association wrote.
New York was the 49th state to implement Medicaid coverage of ABA. The full Medicaid benefit for ABA, which was approved by the Legislature, has not yet been implemented. — New York State Association for Behavior Analysis, testimony submitted to the New York State Legislature, 2025
The Rate History: From $7.25 to $19.07 to $14.45
New York’s ABA Medicaid rate history tells the story of a program built under pressure and now being unwound before it has matured. When the state launched the FFS benefit in August 2021, it set the initial reimbursement for ABA services at $7.25 per 15-minute unit — equivalent to $29.00 per hour. That rate was, at the time of launch, among the lowest initial rates for a newly enacted ABA Medicaid benefit in the country. It placed New York at an immediate competitive disadvantage in attracting providers and LBAs from neighboring markets in New Jersey, Connecticut, and Massachusetts, where Medicaid and commercial rates were materially higher.
On April 1, 2022, New York raised the FFS rate substantially, to $19.07 per 15-minute unit — $76.28 per hour — and automatically reprocessed all pending claims at the new rate. The increase represented a 163 percent improvement from the launch rate and brought New York closer to a nationally competitive position for the 97153 code. At the same time, effective January 1, 2023, New York moved ABA services into the Medicaid Managed Care benefit package, requiring LBAs providing services to MMC enrollees to be credentialed by each enrollee’s specific managed care plan.
The April 2022 rate increase, combined with the 2022 change allowing BCBAs to qualify for LBA licensure through a streamlined second pathway, were the two most significant pro-market actions the state took in its brief history of ABA Medicaid coverage. Both arrived after years of advocacy and after the program had already launched at rates too low to attract the provider base needed to serve the existing demand. The two-step cut from $19.07 to $14.45 between October 2025 and April 2026 erases more than 70 percent of the 2022 rate increase, while the structural challenges that limited program uptake in the first place remain largely unresolved.
The LBA Shortage: A Structural Problem Decades in the Making
The rate crisis in New York is inseparable from the workforce crisis that preceded it. New York has both a licensed behavior analyst statute — the LBA license, administered by the New York State Education Department under Article 167 of the Education Law — and a certified behavior analyst assistant credential (CBAA). Under New York law, only LBAs and CBAAs, and certain exempt licensed professionals, may legally practice ABA. This created a state-specific credentialing requirement that functioned as a supply gate for the national BCBA workforce.
Until November 2022, New York did not accept the national Behavior Analyst Certification Board examination as a direct pathway to LBA licensure. BCBAs who had trained and practiced in other states could not straightforwardly transfer their credential into New York practice without navigating a separate NYSED application process that did not recognize the national exam. A temporary grandfathering path that had existed from January 2014 through January 2016 was long closed. The NYS Department of Health’s own Evidence Based Benefit Review Advisory Committee, in a July 2025 evidence review, cited this policy as a documented contributor to New York’s provider shortage.
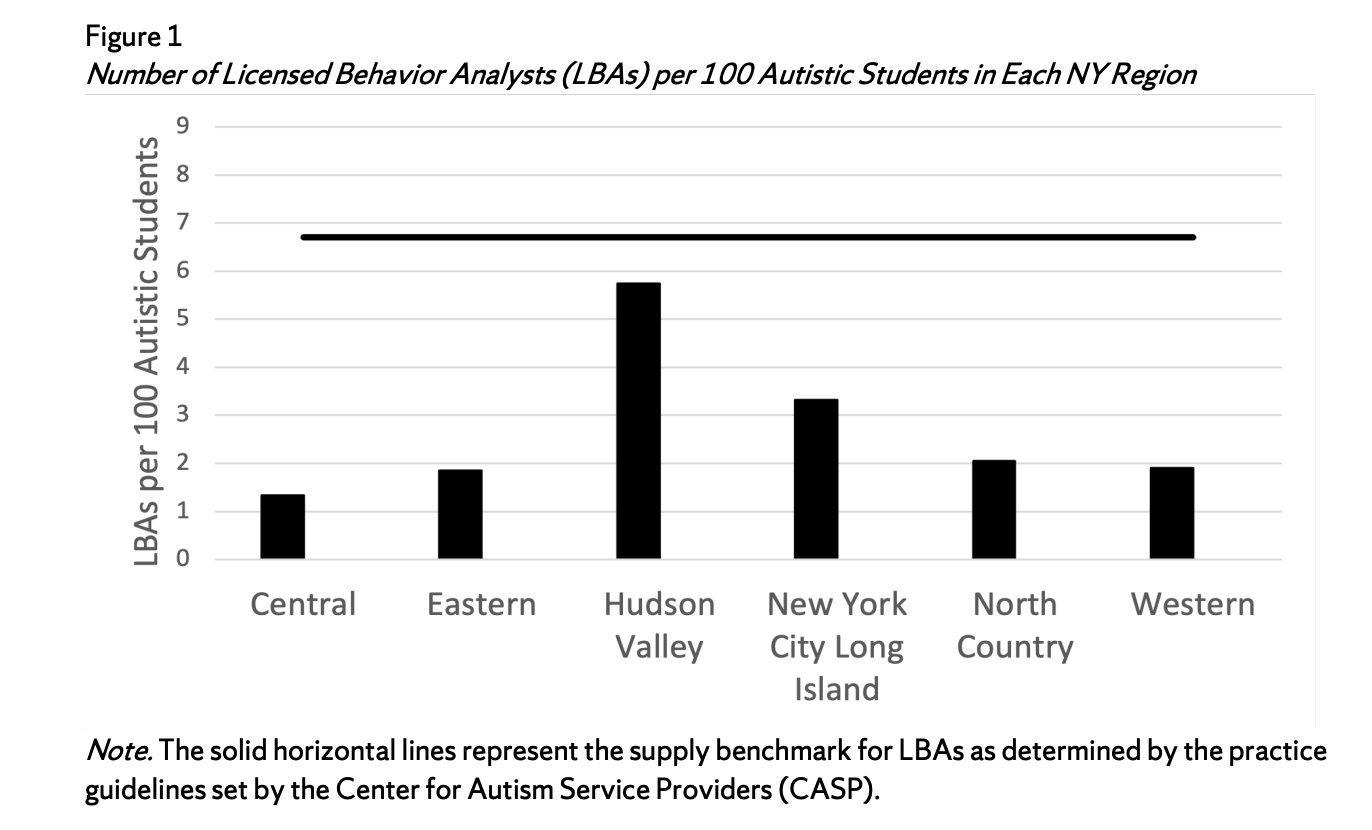
The chart above illustrates the result. The aggregate per capita supply of LBAs per 100 students with ASD in 2022 was 3.2 statewide — less than half of the supply benchmark of 6.67 established by the Council of Autism Service Providers. The Central region, which includes Syracuse and surrounding upstate communities, sits at approximately 1.4 LBAs per 100 ASD students — less than one-quarter of the required minimum. The Eastern and Western regions, which include Albany-area and Buffalo-area communities respectively, hover near 1.9. Even the Hudson Valley, the best-supplied region in the state, falls short of the benchmark at approximately 5.8. No region meets the CASP standard. Because the study underlying the chart was limited to school-aged children with individualized education plans, the NYS DOH evidence review noted that the true shortage across all ASD individuals in New York is likely higher than these figures indicate.
New York’s supervision requirements add complexity beyond the licensure gap. LBAs are required to supervise unlicensed individuals providing behavior analysis services for a minimum of five percent of the hours the unlicensed individual works each calendar month, with at least two face-to-face, real-time contacts per month. The LBA must observe the unlicensed individual providing services in at least one of the monthly meetings. An LBA can supervise no more than six CBAAs at a time. These supervision ratio requirements mean that a small LBA workforce creates a strict ceiling on total service delivery capacity, regardless of the number of unlicensed technicians available to work.
The aggregate per capita supply of LBAs per 100 students with ASD in New York in 2022 was 3.2 — less than half the CASP benchmark of 6.67. No region of the state met the minimum supply benchmark. — NYS DOH Evidence Based Benefit Review Advisory Committee, July 2025
OPWDD: The Parallel System That Governs Much of What ABA Touches
No analysis of New York’s ABA market is complete without understanding the Office for People With Developmental Disabilities, which functions as a parallel state agency coordinating services for individuals with intellectual and developmental disabilities, including autism. As of March 2024, OPWDD coordinates supports for approximately 130,000 people with IDD in New York. Most OPWDD-specialized IDD services are paid through Medicaid fee-for-service, while approximately 38,615 individuals with IDD are enrolled in mainstream Medicaid Managed Care plans for medical and behavioral health services.
OPWDD operates through its own Front Door eligibility process, Care Coordination Organizations, and regional Developmental Disabilities Regional Offices. For a family navigating autism services in New York, the system presents two separate bureaucratic pathways: the DOH-administered ABA Medicaid benefit, which covers ABA for individuals under 21 with ASD or Rett syndrome, and the OPWDD system, which coordinates a broader range of developmental disability services that may include ABA but is governed by separate eligibility criteria, application processes, and oversight structures. The two systems do not share an intake, and movement between them requires separate applications and assessments.
This dual structure has consequences for families in underserved areas. In the Bronx, the OPWDD regional office serves one of the most densely populated and economically stressed autism communities in the state. In Buffalo and the broader Western New York region, the combination of LBA shortages, managed care network contracting gaps, and rural population dispersion creates access conditions that advocates have described as a de facto care desert for Medicaid-dependent families. OPWDD conducted a managed care assessment, published in September 2024 in collaboration with consulting firm Guidehouse, examining a potential transition of OPWDD services to managed care. The report found that survey respondents — primarily family members of people with IDD from the New York City metro region — generally did not report problems accessing existing services, a finding that does not capture the experience of families who have not yet been able to enter the system at all.
The Federal Pressure Layer: OBBBA and What It Means for New York
New York’s state-level ABA rate cuts arrived amid a federal fiscal environment that is simultaneously compressing the state’s overall Medicaid budget. The One Big Beautiful Bill Act, signed into law July 4, 2025, imposes an estimated $900 billion in federal Medicaid reductions over ten years nationally. For New York, the Fiscal Policy Institute estimates the total impact on the state’s healthcare system at a figure far closer to Governor Hochul’s pre-passage estimate of $13 billion annually than to the $3 billion figure the state’s budget director advanced after passage. A critical component of the gap: the state’s MCO tax was projected to generate $3.7 billion in federal revenue for FYs 2026–27, supporting nearly $700 million per year in Medicaid provider rate increases. That revenue is now projected to be cancelled, and those rate increases will not materialize.
For ABA providers in New York, the OBBBA implications compound the state-level rate reduction. The law’s provisions include work requirements for non-disabled Medicaid adults, more frequent eligibility redeterminations, and restrictions on coverage for non-citizen populations. The Essential Plan, which covers more than 1.7 million New Yorkers, faces the elimination of federal funding for approximately 730,000 legally present immigrants beginning in 2027. Families in this population who currently access ABA services through Medicaid will face coverage disruption at the same time that the rate paid to their providers is being reduced.
A bill introduced in the New York State Senate, SB S5107, would add a 680-hour-per-year cap on ABA services under Medicaid — approximately 13 hours per week — while also expanding the definition of treatments for autism spectrum disorder to include DIR-Floortime. If enacted, the cap would formalize the already-operating reality for many Medicaid-dependent families who cannot access their authorized hours due to LBA shortages and managed care network gaps. It would also add a statutory constraint on top of the market constraint, making New York’s effective service ceiling among the most restrictive in the country.
The policy trajectory in New York is, in structural terms, the inverse of the trajectory in states that built their ABA markets through high initial reimbursement rates. New York entered its ABA Medicaid program late, with rates too low to attract a provider base, raised rates after years of advocacy, and is now retreating from those rates before the provider base has stabilized or the full benefit has been implemented. The families in the Bronx and Buffalo waiting years for services are the visible end of a supply chain that the state has consistently failed to price appropriately — and is now pricing down further.
AT A GLANCE
NY ABA Medicaid launch date: August 1, 2021 (FFS); October 1, 2021 (MMC) — the 49th state to implement the benefit
Initial 97153 rate at launch: $7.25 per 15-minute unit ($29/hour) — among the lowest initial rates nationally
Rate after April 2022 increase: $19.07 per unit ($76.28/hour) — a 163% increase; claims auto-reprocessed
97153 rate as of Oct. 1, 2025: $16.85 per unit (FFS); Dec. 1, 2025 for MMC — authorized by NYS Budget FY2025–26
97153 rate as of Apr. 1, 2026: $14.45 per unit ($57.80/hour) — below national average; erases >70% of the 2022 increase
State budget ABA cuts (NYSABA): $9.6M cut FY2025–26; $19M cut FY2026–27 — opposed by New York State Association for Behavior Analysis
LBA supply vs. benchmark (statewide): 3.2 LBAs per 100 ASD students (2022) vs. CASP benchmark of 6.67 — no region of NY met the benchmark
Central NY (Syracuse region): ~1.4 LBAs per 100 ASD students — approximately 21% of the required minimum supply
Best-supplied region (Hudson Valley): ~5.8 LBAs per 100 ASD students — still below the 6.67 CASP benchmark
NY per capita LBA ranking (NE): Lowest in the Northeast as of 2020 (NYS DOH EBBRAC evidence review, July 2025)
National BCBA exam accepted for LBA: Not accepted until November 2022; prior to that, separate NYSED pathway suppressed supply for years
LBA supervision ratio limit: One LBA may supervise no more than 6 CBAAs; minimum 5% monthly supervision of unlicensed staff
OPWDD population served: ~130,000 people with IDD as of March 2024; services primarily through Medicaid FFS
NY Senate ABA cap bill: SB S5107 proposes 680 hours/year cap (~13 hrs/week) and opens autism treatment to include DIR-Floortime
SOURCES & REFERENCES
1. – New York State Medicaid Update. August 2025, Volume 41, Number 8. NYS DOH. health.ny.gov. (CPT 97153 rate cut to $16.85 effective Oct. 1, 2025; $14.45 effective Apr. 1, 2026; authorized by NYS Enacted Budget FY2025–2026.)
2. – New York State Medicaid Update. July 2021, Volume 37, Number 9. NYS DOH. health.ny.gov. (ABA FFS benefit launched August 1, 2021; initial $7.25 rate; LBA/CBAA enrollment requirements.)
3. – New York State Medicaid Update. September 2022, Volume 38, Number 10. NYS DOH. health.ny.gov. (Rate increase from $7.25 to $19.07 per unit effective April 1, 2022; MMC carve-in announcement for January 1, 2023.)
4. – New York State Association for Behavior Analysis (NYSABA). Letter to the Legislature opposing cuts to Medicaid ABA services. February 2025. Filed with the New York State Senate. nysenate.gov. (49th state; $9.6M FY25–26 cut; $19M FY26–27 cut; full benefit not yet implemented.)
5. – NYS DOH Evidence Based Benefit Review Advisory Committee (EBBRAC). “Applied Behavior Analysis Provided Via Telehealth: Evidence Review.” July 2025. health.ny.gov. (Figure 1: LBA supply by NY region vs. CASP benchmark 6.67; statewide 3.2 per 100 ASD students; lowest per capita in Northeast 2020; 2022 BCBA exam acceptance note.)
6. – Council of Autism Service Providers. “50 States Applied Behavior Analysis Medicaid Benefit Comparison.” July 31, 2024. (National rate comparison; Nebraska $36.11 highest rate.)
7. – NYS DOH / eMedNY. Applied Behavior Analysis Policy Manual (2024 version). emedny.org. (LBA/CBAA licensure requirements; supervision ratio rules; billing guidance; school setting exclusion; MMC guidance.)
8. – NYS Office of the Professions, NYSED. “Guidance on the Roles of Licensed Providers and Unlicensed Personnel in Delivering ABA Services.” op.nysed.gov. (Education Law §8803; LBA scope of practice; CBAA scope; unlicensed personnel roles.)
9. – Applied Behavior Analysis Education. “Licensed Behavior Analyst in New York.” Updated February 2026. appliedbehavioranalysisedu.org. (LBA pathway history; Pathway Two for BCBAs opened November 2022; grandfathering closed January 2016.)
10. – Autism Business News / Behavioral Health Business. “State Issues to Watch in Autism Therapy: ABA Hour Caps, Rate Cuts.” March 3, 2025. bhbusiness.com. (NY Senate Bill S5107; 680-hour/year cap proposal; DIR-Floortime inclusion.)
11. – OPWDD / Guidehouse. “New York State Office for People With Developmental Disabilities — Managed Care Assessment Final Report.” September 6, 2024. opwdd.ny.gov. (130,000 people with IDD as of March 2024; 38,615 in mainstream MMC; stakeholder findings.)
12. – Fiscal Policy Institute. “The State Is Understating Threats to NYS Medicaid After OBBBA.” July 25, 2025. fiscalpolicy.org. (MCO tax $1.6B loss FYs26–27; $700M/year in planned provider rate increases will not materialize.)
13. – American Psychological Association. “Update on Cuts to Medicaid Funding.” apa.org. (OBBBA signed July 4, 2025; 11.8 million projected to lose Medicaid nationally; CBO estimates; work requirements.)
14. – Governor Kathy Hochul. Press release: “Governor Hochul Unveils Devastating Impacts of Republicans’ ‘Big Ugly Bill’ on New York State.” governor.ny.gov. (1.5 million New Yorkers projected to lose coverage; $13 billion fiscal impact estimate; 730,000 Essential Plan enrollees at risk.)
15. – New York State Comptroller Thomas DiNapoli. “DiNapoli: Rural Counties Face Shortage of Health Professionals.” August 7, 2025. osc.ny.gov. (Rural NY healthcare deserts; mental health practitioners 6.9 per 10,000 vs. state average 16.1.)