The Mechanics of the Cap
INDIANAPOLIS — The 4,000-hour lifetime cap emerged from a working group that Governor Mike Braun created by executive order in early 2025 to address rapidly rising Medicaid costs while maintaining access to ABA therapy. The working group — comprising nearly two dozen state leaders, health professionals, and stakeholders — delivered its recommendations in November 2025 after months of analysis. The group concluded that ABA spending growth was unsustainable and that gaps in oversight and inconsistencies in billing practices were contributing to rising costs.
The FSSA bulletin issued February 26, 2026 outlined the new framework. The lifetime cap of 4,000 hours takes effect April 1, 2026. For purposes of calculating time in treatment, the clock starts on the effective date of the State Plan Amendment regardless of how many hours a child has already received — meaning that children currently in treatment will be able to continue services for at least 36 months from the SPA effective date. Following the three-year limitation, individuals may still qualify for limited-hour, behavior-specific focused ABA based on medical necessity. Prior authorization with peer review may be required for individuals receiving services for two or more years.
The cap represents a calculation about treatment intensity and duration. At 30 hours per week — a common authorization level for children receiving comprehensive ABA — 4,000 hours would be exhausted in approximately 133 weeks, or roughly two and a half years. At 40 hours per week, the cap would be reached in 100 weeks, or under two years. For children who entered ABA therapy at age three and received intensive services, the cap could be reached before they enter elementary school. The practical effect is to impose a time limit on the most intensive phase of ABA treatment.
The working group also recommended that parents be required to engage in their children’s therapy, proposing 9 to 18 hours of coaching or training per six-month authorization period. FSSA Secretary Mitch Roob framed the requirement directly: if the taxpayer is spending that much money helping a child, the parent or caregiver needs to be engaged. He observed that ABA therapy is usually done outside the home, meaning the parent can choose to be less engaged. The parental engagement mandate reflects a clinical philosophy that ABA outcomes are improved when caregivers implement behavioral strategies in natural settings — and a fiscal philosophy that the state should not be paying for full-time therapy if parents are not participating.
If the taxpayer is spending that much money on helping this child, we believe that parent or caregiver needs to be engaged. — FSSA Secretary Mitch Roob
How Indiana Compares
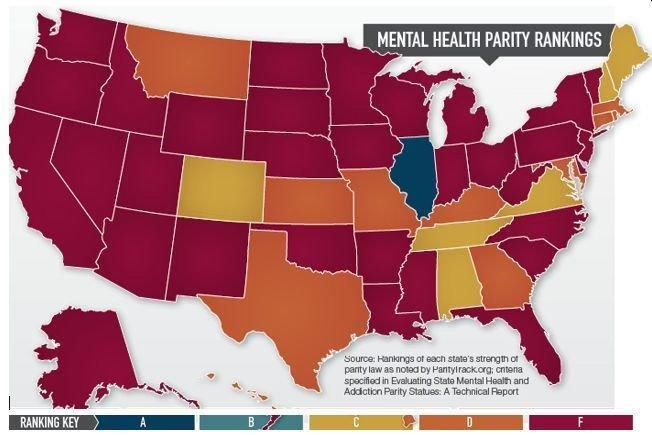
Indiana’s 4,000-hour lifetime cap is the most restrictive in the country, but it exists on a spectrum of state-level ABA utilization controls that is tightening nationwide. Nebraska cut Medicaid ABA payments by up to 80 percent. Colorado is implementing pre-payment review and post-payment auditing. New York is considering legislation that would impose similar cost controls. The pattern is clear: states are moving from open-ended ABA authorization to managed, capped, and monitored utilization models.
The cap must also be understood in the context of Indiana’s prior OIG audit findings. The 2024 OIG audit of Indiana’s 2019 and 2020 ABA payments found $56 million in confirmed improper payments and an additional $78 million in potentially improper payments, with a $39.4 million refund recommendation. The working group’s report pointed to these findings as evidence that the prior system was not only expensive but poorly controlled. The 4,000-hour cap is, in part, a response to an audit trail that demonstrated the state was paying for services it could not verify were properly delivered.
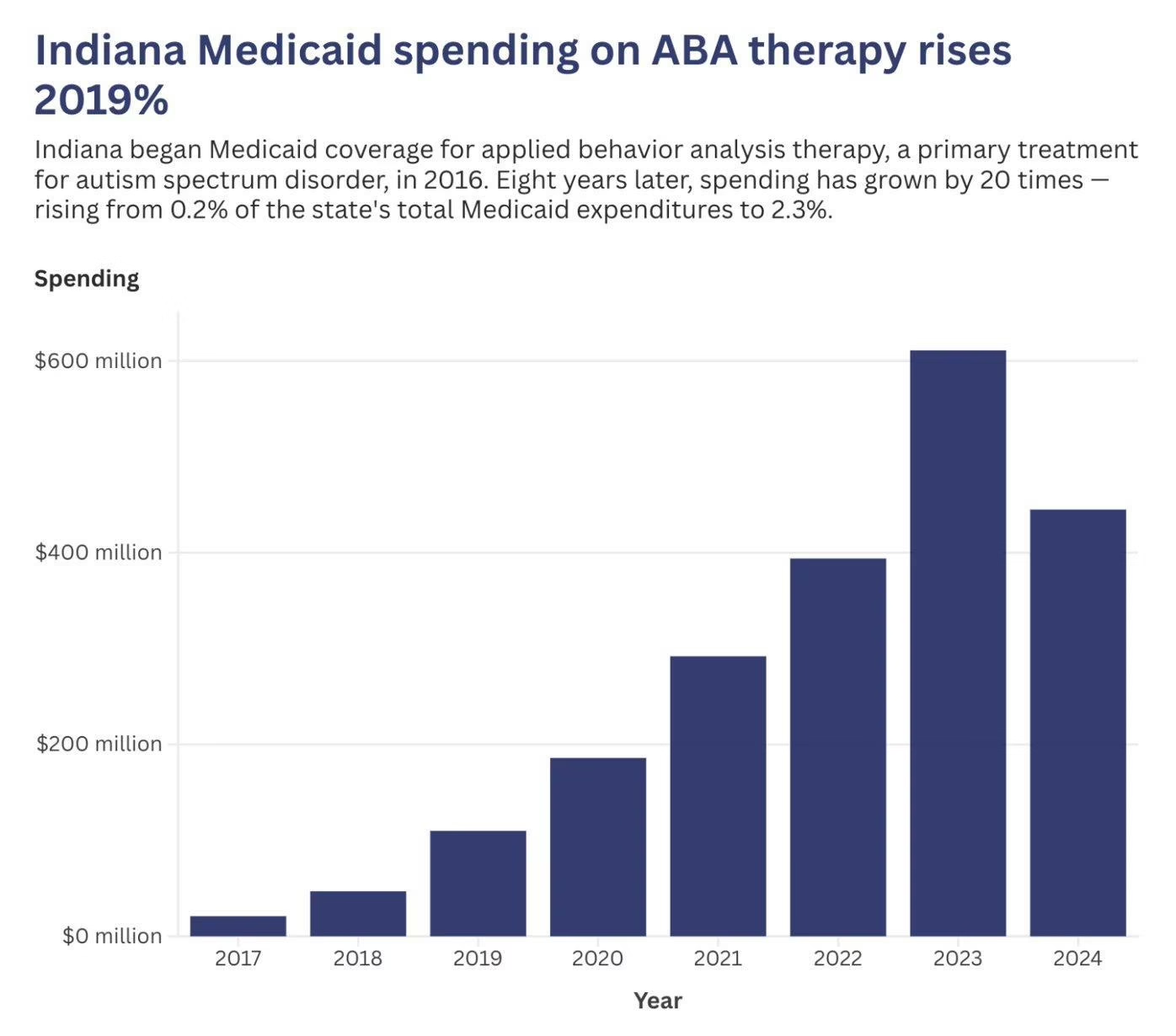
The working group’s package of recommendations is projected to reduce the annual ABA spending growth rate from approximately 13 percent to 7 to 8 percent, though no specific dollar savings estimate has been released. Without intervention, costs were projected to reach an estimated $825 million by 2029. Roob emphasized that the state serves 1.8 million people through Medicaid and cannot make decisions about ABA in a vacuum.
FSSA is creating a dedicated ABA program office within the agency to manage the benefit as a program rather than a claims-processing function. The office will have staff with clinical expertise and the authority to implement utilization management, quality monitoring, and fraud prevention. Roob described the current structure as inadequate: the Office of Medicaid Policy and Planning’s job is to pay claims. They’re not told to be managing a program. The new office represents a shift from passive claims payment to active program management.

The Advocacy Response
Advocates for children with autism and developmental disabilities have expressed concern that the 4,000-hour cap will harm children who need extended intensive treatment. Kim Dodson, CEO of the Arc of Indiana, applauded the administration’s crackdown on fraudulent billing but expressed concern that enforcement actions could hurt services for children who genuinely need ABA therapy. The tension between fraud enforcement and access preservation is the central challenge facing every state that is reforming its ABA program.
The parental engagement mandate has drawn particular scrutiny from working families who argue that requiring 9 to 18 hours of coaching per six-month period is unrealistic for parents who hold full-time jobs, care for other children, or face transportation barriers. The mandate assumes a level of parental availability that may not exist in the Medicaid population, which by definition includes families with limited financial resources.
For the national ABA industry, Indiana’s cap is a leading indicator. If the cap produces the projected cost savings without generating significant political backlash, other states will adopt similar models. If the cap produces documented harm to children — measured in regression, emergency department visits, or school performance — it will become a cautionary tale. Indiana is running the experiment that every other state is watching, and the results will shape ABA policy for years to come.
AT A GLANCE
| Lifetime cap: | 4,000 hours; effective April 1, 2026 |
| After cap exhausted: | 15 hours/week if medically necessary; prior authorization with peer review |
| Treatment duration limit: | 36 months of comprehensive ABA from SPA effective date |
| Rate changes: | Phasedown of reimbursement rates; effective April 1, 2026 |
| Parental engagement: | 9–18 hours coaching/training per 6-month authorization |
| Medicaid ABA enrollees: | 8,000+ Hoosiers; most ages 3–8 |
| Cost projection: | 25M by 2029 without intervention; growth reduced from 13% to 7–8% |
| Prior OIG audit: | 6M improper + 8M potentially improper; 9.4M refund |
| New program office: | Dedicated ABA office within FSSA with clinical expertise |
| Other reforms: | Provider moratorium, accreditation requirement (timeline TBD) |
SOURCES & REFERENCES
| 1. | Indiana Capital Chronicle. “State coming down on ABA providers that potentially abused system.” March 24, 2026. |
| 2. | Indiana Capital Chronicle. “Governor’s group recommends ABA usage cap, rate changes.” November 12, 2025. |
| 3. | FSSA. “Applied Behavioral Analysis therapy services.” in.gov/fssa. February 26, 2026 bulletin. |
| 4. | Axios. “Medicaid autism therapy boom triggers crackdown.” March 16, 2026. |
| 5. | Wall Street Journal. “The Boom in Autism Therapy Is Medicaid’s Fastest-Growing Jackpot.” March 10, 2026. |








Join the discussion ▾