Demand Without Providers
ACROSS THE UNITED STATES — Autism prevalence does not follow a geographic path. One in 31 children is now diagnosed, in cities, suburbs, and farm counties alike. The workforce that treats it does follow a map, and the map is stark: recent analyses of BACB certificant data put the share of US counties without a single Board Certified Behavior Analyst at roughly half, and a TYGES analysis estimates the country would need about five times its current BCBA workforce to meet demand.
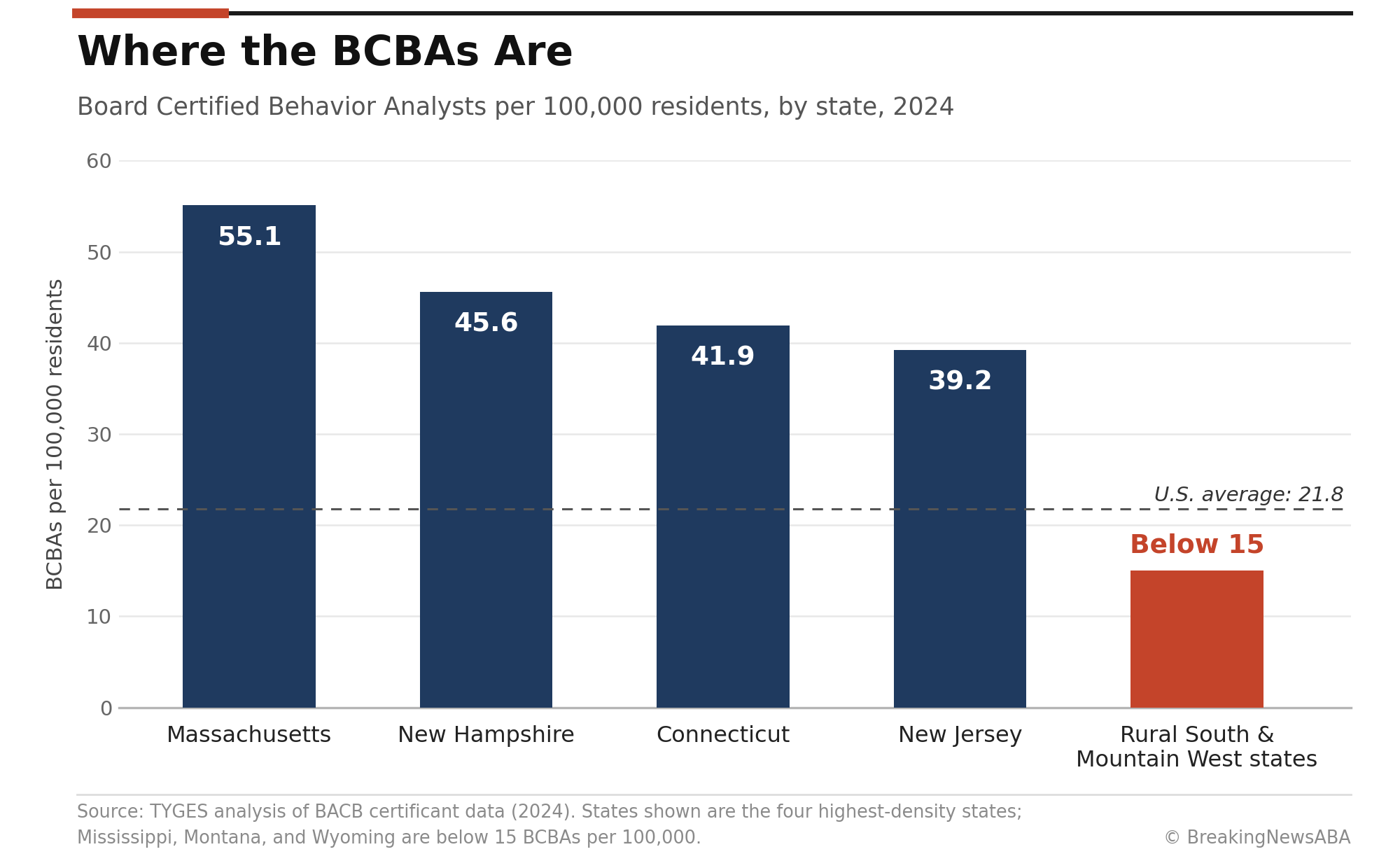
The maldistribution shows up in the state figures. Massachusetts has 55.1 BCBAs per 100,000 residents; New Hampshire, Connecticut, and New Jersey all sit above 39. States across the rural South and Mountain West, including Mississippi, Montana, and Wyoming, are below 15, and many of their counties have zero. The pattern is not new: a 2021 peer-reviewed study found that affluent metropolitan counties had by far the highest access to BCBAs, and a 2022 follow-up analysis by the same research team found that as of 2021, 37.4 percent of counties had no BCBAs and 8.2 percent had none in the county or any bordering county.
Meanwhile, capital has kept buying where the clinicians already are. Private equity acquired roughly 500 autism therapy centers over the past decade, nearly all in urban markets, a concentration BreakingNewsABA examined in June as middle-market investors began circling the rural gap. Rural America, home to about one in five Americans and spanning 97 percent of the country’s land area, is the last large unserved ABA market. The question the whole industry keeps circling is whether anyone can serve it profitably.
Why the Economics Break
The rural P&L fails in predictable places. Caseload density is the first: an RBT who spends ninety minutes driving between two clients delivers fewer billable hours per day than an urban peer, and mileage, drive time, and cancellations across long distances land directly on margin. Recruiting is the second: BCBA job postings hit 132,307 in 2025, up 28 percent, against roughly 83,600 active BCBA certificants, and in that market, a clinician weighing offers rarely chooses the town without an airport. Employers in shortage areas are already paying sign-on bonuses and relocation packages to compete.
Payer mix is the third and heaviest weight. Rural caseloads skew toward Medicaid, and in low-rate states, Medicaid reimbursement of $40 to $55 an hour leaves practices struggling to clear 12 to 15 percent EBITDA margins, roughly half of what commercial-heavy urban practices earn, per valuation benchmarks published by YourExitValue. A model that is thin at urban density gets thinner with every empty mile between sessions. That arithmetic, more than any lack of demand, is why the private-equity map and the BCBA map look the same.
The Models Being Tested
Telehealth is the lever every new entrant is pulling, in different amounts. At the pure end, AnswersNow raised a $40 million Series B in January to scale a fully virtual, BCBA-delivered model with no RBTs; the Richmond, Virginia, company says it delivered nearly 100,000 hours of virtual therapy and caregiver training in 2025 and claims payer savings of up to 75 percent compared with traditional care. Forta Health markets Medicaid-covered virtual ABA to rural families in multiple states, pairing remote clinicians with active parent coaching. These models treat geography as irrelevant: the BCBA can live anywhere.
Between fully virtual and fully local sit the hybrid designs most operators consider more durable for intensive cases: a remote BCBA supervising local RBTs hired in the community, periodic in-person visits layered over regular telehealth sessions, mobile teams rotating through a circuit of small towns, and school partnerships that use existing buildings and existing daily attendance instead of new centers. Each variant attacks a specific rural cost, supervision travel, facility overhead, or family drive time, while keeping hands-on delivery local.
The caveats are real. Telehealth-heavy models lean on caregiver mediation, which does not fit every child, every severity level, or every family’s capacity. Medicaid coverage of telehealth ABA varies by state and remains subject to the same rate pressure squeezing the rest of the benefit. And the virtual segment has already produced failures alongside its funding rounds, a reminder that access and unit economics are not the same achievement.
Incentives, and the Hole in Them
Health care has a standard toolkit for exactly this problem: pay clinicians to go where the patients are. The National Health Service Corps offers behavioral health providers up to $50,000 in loan repayment for a two-year commitment in a shortage area, and up to $100,000 over three years in its substance-use-focused rural program. But behavior analysts are not among the NHSC’s eligible behavioral health disciplines, which include psychiatrists, psychologists, clinical social workers, marriage and family therapists, and licensed professional counselors. The main federal engine for moving clinicians into rural shortage areas simply does not include the profession that treats autism.
State-run loan repayment programs, which HRSA funds through cost-sharing grants, give each state discretion over eligible disciplines; whether a behavior analyst qualifies depends entirely on the state. Licensure portability is a second structural gap. Forty US jurisdictions license or register behavior analysts, each separately, and, unlike counselors, psychologists, social workers, and speech-language pathologists, behavior analysts have no interstate licensure compact. The Counseling Compact is live in six states, and the speech-language compact began issuing privileges in October 2025. For a telehealth-first ABA model whose entire premise is that the BCBA can live anywhere, a 40-license patchwork is a tax on the one design that scales in rural markets.
The federal government pays psychologists and counselors to move to shortage areas. Behavior analysts are not on the list.
What Would Have to Be True
The rural opportunity is real and not going away: the demand is diagnosed, mandated, and largely unserved. For the economics to work, some combination of four things has to hold. Telehealth reimbursement must remain at or near parity in Medicaid programs. Hybrid staffing has to keep the expensive clinician remote and the local labor local. Incentive programs, federal or state, have to start treating behavior analysts like the shortage profession the data says they are. And licensure has to get more portable, whether through a compact or state-by-state reciprocity, so one BCBA can legally serve families across the multi-state regions where the deserts actually sit.
None of those four is exotic, and each has a working precedent in an adjacent profession. Which is why the investors now studying the rural map are less interested in whether rural ABA can pay than in who gets the model right first. In a field where more than half the counties are still empty, the first operator with durable rural unit economics is not competing for market share. It is the market.
AT A GLANCE
| US counties without a BCBA: | Roughly half, per analyses of BACB certificant data (TYGES; BACB) |
| Workforce gap: | ~5x the current BCBA workforce needed to meet estimated demand |
| 2025 demand signal: | 132,307 BCBA job postings, up 28% (BACB/Lightcast), vs. ~83,600 active BCBAs |
| Density spread: | Massachusetts 55.1 BCBAs per 100K; Mississippi, Montana, Wyoming below 15 |
| Peer-reviewed baseline: | 37.4% of counties had no BCBA (2021 data, 2022 follow-up study); access highest in affluent metro counties (2021 study) |
| Rural market size: | ~1 in 5 Americans across 97% of US land area (Census) |
| Rural margin pressure: | Low-rate Medicaid ($40–$55/hr) practices struggle to clear 12–15% EBITDA |
| Telehealth capital: | AnswersNow $40M Series B (Jan 2026); ~100,000 virtual hours in 2025 |
| Incentive gap: | BCBAs not among NHSC-eligible behavioral health disciplines (up to $50K–$100K for others) |
| Licensure gap: | 40 jurisdictions license behavior analysts; no interstate compact, unlike counseling, psychology, social work, SLP |
| PE footprint: | ~500 autism centers acquired in a decade, nearly all urban |
SOURCES & REFERENCES
| 1. | BreakingNewsABA. “Half of U.S. Counties Have No BCBA. Demand Hit 132,307 Job Postings in 2025. Can Telehealth Close the Gap?” April 4, 2026. https://breakingnewsaba.com/industry-analysis/half-of-u-s-counties-have-no-bcba-demand-hit-132307-job-postings-in-2025-can-telehealth-close-the-gap |
| 2. | TYGES. “Applied Behavioral Analysis (ABA) Care Deserts in the U.S.: A State-by-State Look at BCBA Shortages” (state density figures from BACB certificant data). 2026. https://tyges.com/healthcare-practice/behavioral-health-care-deserts/ |
| 3. | Yingling et al. “Impact of County Sociodemographic Factors and State Policy on Geographic Access to Behavior Analysts Among Children with Autism Spectrum Disorder” (2021) (affluence odds ratios), https://pubmed.ncbi.nlm.nih.gov/33620610/; and “Trends in Geographic Access to Board Certified Behavior Analysts Among Children with Autism Spectrum Disorder, 2018–2021” (2022) (37.4% of counties with no BCBAs; 8.2% with none in county or bordering counties), https://pmc.ncbi.nlm.nih.gov/articles/PMC8727480/ |
| 4. | CertifyndABA. “BCBA Job Outlook 2026” and “How Much Does a BCBA Make in 2026?” (83,586 active BCBAs; 1.6 openings per BCBA; 266 counties gained first BCBA 2018–2021; rural sign-on bonuses). 2026. https://certifyndaba.com/blog/career-development/bcba-job-outlook-2026 and https://certifyndaba.com/blog/salary-compensation/how-much-does-a-bcba-make-2026 |
| 5. | BreakingNewsABA. “Middle Market PE and Venture Capital Explore Rural Therapy-Care Deserts” June 3, 2026. https://breakingnewsaba.com/private-equity-in-aba/middle-market-pe-and-venture-capital-explore-rural-therapy-care-deserts |
| 6. | YourExitValue. “ABA Therapy Business Valuation Calculator & Exit Planning” (Medicaid low-rate margin benchmarks). https://www.yourexitvalue.com/industries/aba-therapy |
| 7. | HLTH. “AnswersNow Raises $40M Series B to Scale AI-Enabled, BCBA-Led Virtual Autism Therapy” (round details; 2025 volume; payer-savings claims). January 22, 2026. https://hlth.com/insights/news/answersnow-raises-40m-series-b-to-scale-ai-enabled-bcba-led-virtual-autism-therapy-2026-01-22 |
| 8. | Forta Health. “Virtual ABA for Rural Families: Bringing Expert Autism Care Home” (Medicaid-covered virtual model; rural focus). https://www.fortahealth.com/resources/virtual-aba-for-rural-families-bringing-expert-autism-care-home |
| 9. | LinksABA. “ABA in Rural Areas: Access, Telehealth, and Equity” (rural population/land share per Census; hybrid, mobile, and school-partnership models). 2025. https://linksaba.com/aba-in-rural-areas-access-telehealth-and-equity/ |
| 10. | National Health Service Corps (HRSA). “NHSC Loan Repayment Program” and “NHSC Rural Community Loan Repayment Program” (award amounts; eligible disciplines). 2026. https://nhsc.hrsa.gov/loan-repayment/nhsc-loan-repayment-program and https://nhsc.hrsa.gov/loan-repayment/nhsc-rural-community-loan-repayment-program |
| 11. | North Carolina DHHS, Office of Rural Health. “Medical, Dental, and Psychiatric Recruitment Opportunities” (NHSC-eligible behavioral health disciplines list). https://www.ncdhhs.gov/divisions/office-rural-health/office-rural-health-programs/provider-recruitment-and-placement/medical-dental-and-behavioral-health-recruitment-and-incentives |
| 12. | Counseling Compact Commission (compact live in AZ, GA, IN, LA, MN, OH, June 2026), https://counselingcompact.gov/; behavior analyst licensure landscape (40 jurisdictions): AppliedBehaviorAnalysisEDU, https://www.appliedbehavioranalysisedu.org/state-by-state-guide-to-aba-licensing/ |
| 13. | Centers for Disease Control and Prevention. “Data and Statistics on Autism Spectrum Disorder” (1 in 31 children aged 8 identified with ASD; ADDM Network, 2022 data). https://www.cdc.gov/autism/data-research/index.html; primary surveillance report (MMWR, April 2025): https://www.cdc.gov/mmwr/volumes/74/ss/pdfs/ss7402a1-H.pdf |
| 14. | National Governors Association. “Understanding Behavioral Health Licensure Compacts” (Counseling, PSYPACT, and Social Work as the behavioral health compacts; no behavior analyst compact). https://www.nga.org/publications/understanding-behavioral-health-compacts/; ASLP Interstate Compact issuing privileges from October 2025: https://www.speechpathologygraduateprograms.org/blog/the-interstate-compact-is-coming/ |