WASHINGTON, D.C. — In 2014, the Centers for Medicare and Medicaid Services issued an Informational Bulletin clarifying that states were required to cover medically necessary behavioral health services for children with autism — including Applied Behavior Analysis — under Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment benefit. The bulletin did not mandate ABA specifically, but the practical effect was to open the largest single funding channel the ABA industry would ever see. By 2022, every state Medicaid program in the country covered ABA. That decision, more than any investment thesis or PE roll-up strategy, is what built the modern ABA industry.
And then the money came. According to a December 2025 analysis by Trilliant Health of Medicaid and commercial claims data, total Medicaid spending on ABA procedure codes grew 279 percent from 2018 to 2024, reaching $14.49 billion across all states. ABA visits — individual service encounters — increased 267 percent over the same period, with Medicaid utilization growing 298 percent and commercial utilization growing 249 percent. The number of ABA-related clinicians more than doubled, up 135 percent, with significant variation across states: Nebraska’s ABA workforce grew 761 percent, Wyoming’s declined 32 percent.
The diagnoses followed the coverage. Autism prevalence in the United States has risen from 1 in 150 children in 2000 to 1 in 31 in 2022 — a fourfold increase driven by a combination of expanded diagnostic criteria, better screening, and, critics argue, the financial incentives created by a reimbursement structure that pays per unit of service regardless of outcome. CMS data show that approximately 5 percent of children ages 3 to 17 on public insurance have autism spectrum disorder, compared with 2 percent of commercially insured children. That 2.5 times gap — consistent across multiple data sources — has become one of the most contested numbers in health policy: a sign of appropriately captured unmet need among low-income populations, or a sign that something other than clinical need is driving Medicaid ABA utilization at its current rates.
State budget offices do not resolve that debate. They see a line item that has grown by hundreds of percent in a few years and they reach for the tools they have. Twelve states have taken or proposed significant action on ABA reimbursement since 2023. Federal audit findings have documented improper payments running into the hundreds of millions. The One Big Beautiful Bill Act, signed by President Trump in 2025, includes more than $900 billion in federal Medicaid spending reductions over ten years. The fiscal pressure that created the modern ABA industry is now, in a different form, the defining threat to it.
THE SPENDING NUMBERS: STATE BY STATE
The aggregate $14.49 billion figure obscures the variation in how the spending crisis has landed by state. The most dramatic examples are instructive not because they are typical, but because they reveal the structural dynamics that are now playing out everywhere at different speeds.
Indiana — $611M peak (2023). 2,800% growth (2017–23). Rate cut to $68/hr (2024); proposed 30hr/week cap. Cap pulled back; new tiered approach being developed.
North Carolina — $639M projected (FY2026). 423% growth (FY2022–26). 10% rate cut (Oct. 2025). Preliminary injunction halting cut; lawsuit ongoing.
Nebraska — $85M (2024). 1,700% growth (2020–24). 48% rate cut for direct therapy (Aug. 2025). Providers staying but margins compressed; Above & Beyond reversed exit.
Arizona — $371M (2025). 43% growth in one year. MCO contract terminations (Mercy Care, AZ Complete Health). Two class action lawsuits; Centria case in Maricopa County Superior Court.
Colorado — ~$200M+. Emergency 20% legislative increase (2023); further cuts proposed. Hopebridge exited 2023; lawsuit by providers and parents challenging prior authorization.
Wisconsin — Federal audit: $18.5M improper payments (2021–22). No post-payment reviews conducted since ABA added to Medicaid (2016).
Minnesota — 85 open fraud investigations; FBI raids (2024). Criminal investigations ongoing.
New York — Proposed 680-hour/year cap (SB S5107). Legislation pending; advocacy community mobilized.
Indiana is the most studied case because it arrived first and has been managed most publicly. The state’s Medicaid program began covering ABA in 2016. Spending reached $21 million in 2017 and grew to $611 million in 2023 — a 2,800 percent increase in six years. Indiana’s peculiar reimbursement structure — which historically paid providers 40 percent of whatever they charged, regardless of what they billed — created, as the president of the Indiana Providers of Effective Autism Treatment put it, ‘very strange incentives for a small portion of the provider network.’ Providers charging exorbitant amounts received high reimbursements; the state had no rate discipline mechanism. A 2024 HHS Inspector General report estimated at least $56 million in improper payments in Indiana in 2019 and 2020, with an additional $78 million potentially improper. Providers had billed for excessive hours, including during nap time.
Nebraska’s trajectory was even steeper in relative terms, though from a smaller base. The state spent $4.6 million on ABA through Medicaid in 2020; by 2024, that figure had reached $85 million — an 1,800 percent increase in four years. Nebraska had deliberately set its ABA reimbursement rates above national norms to attract providers to an underserved rural state, and it worked: providers came. Then in August 2025, the Nebraska Department of Health and Human Services cut rates by 48 percent for direct therapy services provided by behavior technicians, from approximately $144 per hour to $74.80. Parent training rates were cut 51 percent; care plan and protocol adjustment rates by 37 percent.
North Carolina’s story is similar in structure but larger in scale and more recent in timing. ABA spending in the state was $122 million in fiscal year 2022 and is projected to reach $639 million in fiscal year 2026 — a 423 percent increase in four years. In October 2025, North Carolina Medicaid cut reimbursement rates for autism services by 10 percent, arguing state legislators had not budgeted enough to cover rising costs. Families of 21 children filed suit immediately; a court issued a preliminary injunction briefly halting the cut. The legal argument — that the rate reduction discriminated against children with disabilities — parallels arguments being made in courtrooms across the country.
THE STRUCTURAL PROBLEM BEHIND THE NUMBERS
The rate of growth in ABA spending, and the variation between Medicaid and commercial utilization, has produced a genuine debate about what is actually driving the numbers. The explanation that most policy researchers favor is a combination of several factors operating simultaneously: legitimate expansion of access to previously unserved populations, increased autism diagnosis rates that partly reflect real changes in prevalence and partly reflect expanded diagnostic criteria, and a reimbursement structure that creates systematic incentives for volume maximization regardless of clinical appropriateness.
“The current payment structure reimburses based on service volume rather than outcomes, creating misaligned incentives. Providers benefit financially from maximizing billable hours regardless of whether treatment produces meaningful improvements in children’s functioning.”
The Trilliant Health analysis articulates the problem directly: the volume-based fee-for-service model that governs ABA reimbursement creates misaligned incentives. The recommendation — which echoes what providers like Cortica and Hopebridge have been arguing for years — is to shift toward value-based reimbursement that ties payment to outcomes rather than encounter counts. The challenge is that value-based care for ABA requires outcome measurement infrastructure that most states do not have and most providers have not been required to build.
The fraud dimension complicates the picture further. Wisconsin’s Medicaid program had conducted no post-payment review of ABA claims since the program began in 2016, according to a federal audit that found at least $18.5 million in improper payments in 2021 and 2022. In Minnesota, state officials had 85 open investigations into autism providers as of late 2025, following FBI raids on two providers as part of a Medicaid fraud investigation involving alleged kickback schemes. Massachusetts reached settlement agreements with two ABA providers over inappropriate billing practices with MassHealth, then implemented an accreditation mandate requiring managed care organizations to contract only with providers accredited by recognized quality bodies — the most structural attempt by any state to use credentialing as a cost-control mechanism.
The fraud and billing irregularity findings do not describe the whole industry. The vast majority of Medicaid ABA spending goes to providers delivering legitimate services to families who have few other options. But the findings do describe a systematic vulnerability in a reimbursement structure that was designed for a different era: pre-authorization protocols written before the scale of ABA utilization was predictable, supervision requirements that vary dramatically by state, and an absence of required outcome reporting that would allow payers to distinguish effective treatment from billing optimization.
HOW STATES ARE RESPONDING: THE TOOLKIT
The tools available to state Medicaid programs attempting to control ABA spending are limited, and each one carries costs that fall on families. Rate cuts are the fastest and most common mechanism. They reduce spending per encounter but can also reduce provider participation, particularly in rural and underserved markets that are already thin on provider supply. Nebraska’s 48 percent rate cut prompted Above and Beyond Therapy — the state’s largest ABA provider, billing more than $28.5 million through the Medicaid managed care program in 2024, roughly a third of the state’s total ABA spend — to announce that it would exit the Nebraska Medicaid network, before reversing course under public pressure. The announcement and reversal within one week illustrated the supply fragility that makes aggressive rate cutting politically as well as clinically risky.
Hour caps attempt to limit spending by constraining utilization rather than price. Indiana has proposed, pulled back, and revised plans to cap ABA coverage at 30 hours per week for a maximum of three years, with the most recent iteration creating tiers based on symptom severity. The 30-hour cap was described by Governor Mike Braun’s own administration as ‘cruel and unusual punishment’ when applied retroactively — the formulation that had led to the proposal’s initial withdrawal. A tiered approach that reserves higher hours for children with greater need is clinically more defensible, but implementing it requires diagnostic and assessment infrastructure that states do not currently have in place, and any cap risks cutting service to children with significant need who happen to fall below the threshold.
Prior authorization requirements, tightened provider enrollment criteria, and accreditation mandates are slower-moving tools that address the structural problem rather than the immediate budget line. Massachusetts’ accreditation mandate — requiring MCO contracted ABA providers to hold BHCOE, CASP, or equivalent accreditation — addresses the quality and oversight gap directly. But it also reduces provider supply in the short term, which can extend wait times for families in markets where supply is already insufficient to meet demand. Indiana’s working group, convened by Governor Braun and reporting recommendations in November 2025, included a temporary moratorium on new ABA therapy sites — an attempt to slow the provider entry that has outpaced oversight capacity.
THE FEDERAL MULTIPLIER
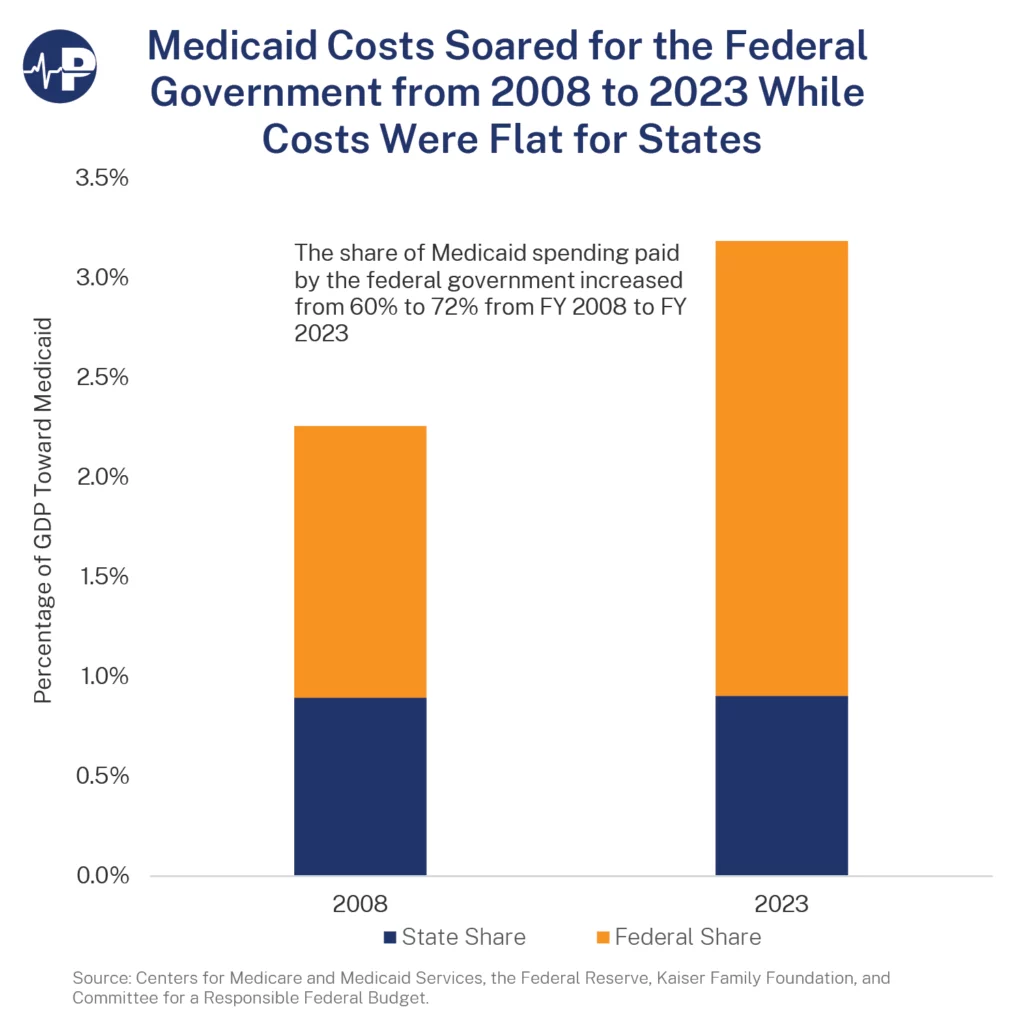
The state-level pressure is significant on its own terms. The federal dimension makes it structural. The One Big Beautiful Bill Act, signed in 2025, includes more than $900 billion in federal Medicaid spending reductions over ten years through a combination of per capita caps on federal matching funds, limits on provider tax financing, and reductions in the Federal Medical Assistance Percentage for expansion populations. The Congressional Budget Office’s preliminary analysis estimated the law will increase the number of uninsured Americans by approximately 7.8 million by 2034.
For ABA specifically, the federal cuts compound state-level pressures in two ways. First, they reduce the federal matching funds that flow to states for every Medicaid dollar spent — which means that states facing growing ABA line items will receive less federal support for the same spending level. Second, they create pressure on state general funds that extend beyond ABA: when total Medicaid costs rise and federal matching declines, states have less discretionary room across the entire Medicaid program, and the fastest-growing line items become the most visible targets for cost control.
Robert F. Kennedy Jr., as HHS Secretary, has described autism as a rapidly growing epidemic and made it a major focus of his tenure. The policy implications of framing autism as an epidemic — rather than as a condition requiring evidence-based support — are contested by disability advocates and clinical researchers. But the framing may affect the political calculus around ABA spending: if autism rates are rising because of an environmental cause that is being investigated, spending $14 billion annually on behavioral therapy for a growing population is framed differently in the policy conversation than if the rising rates reflect better diagnosis of a neurodevelopmental condition that has always been present at higher rates than previously measured.

THE INDUSTRY’S RESPONSE: ADVOCACY, LITIGATION, AND VALUE-BASED CARE
The ABA provider industry has responded to the spending crisis through three overlapping channels. The first is advocacy: providers and families have organized at the state level with significant effect. Capitol rallies in Arizona, Nebraska, and North Carolina in 2025 and 2026 put human faces on what had been framed as an actuarial problem. Parents of children who had made measurable developmental progress under ABA therapy — learning to speak, achieving toilet training, starting school — testified to state legislatures and appeared in media. The family advocacy response has been effective at slowing the pace of cuts in several states and at creating political costs for governors willing to apply them retroactively.
The second channel is litigation. Centria Autism’s December 2025 lawsuit against Mercy Care and AHCCCS in Arizona is the most significant pending case, with its argument that a managed care organization cannot use a for-any-reason termination clause to eliminate the largest providers from its network without triggering federal network adequacy requirements. If the argument prevails, it constrains the ability of MCOs to use provider termination as a rate management tool — a constraint that would have broad implications for every state where Medicaid ABA is administered through managed care. Similar litigation in North Carolina and Colorado is at earlier stages.
The third channel is the push toward value-based care — the argument that the spending crisis is fundamentally a problem of the wrong reimbursement model, and that shifting from volume-based to outcome-based payment would simultaneously reduce unnecessary utilization and demonstrate the clinical value of appropriate ABA. The major integrated providers — Cortica with $255 million raised specifically to build a value-based care model, Hopebridge with its Clinical Advisory Board and outcome data aspirations — have been arguing this case to payers and investors for years. The challenge is that value-based ABA contracting requires agreed-upon outcome measures, measurement infrastructure, and willingness from payers to accept risk-sharing arrangements. As of early 2026, four Cortica value-based contracts exist nationwide. The fee-for-service model is still paying nearly all of the $14.49 billion.
WHAT COMES NEXT
The trajectory of the next three to five years in Medicaid ABA is reasonably predictable in its broad strokes, even if the state-level details remain highly contested. Total spending will not continue to grow at 279 percent per six-year period; the fiscal pressures are too significant and the political visibility too high. The question is not whether the growth rate slows, but how the slowdown is achieved — through rate discipline, utilization controls, outcome-based contracting, fraud elimination, or some combination of all four — and what the consequences are for the families who depend on Medicaid to access services that the private market cannot provide at comparable cost.
The most vulnerable outcomes are in the markets that the industry was designed to serve: rural states with thin provider density, where any significant rate reduction or provider exit reduces access to services for families with no alternative. Nebraska’s August 2025 rate cut, implemented with 30 days’ notice in a state where behavior analysts are scarce and families routinely travel long distances to reach a center, is the model of how not to manage this transition. The warning from Leila Allen of Lighthouse Autism Center — that the state conducted no cost survey before implementing cuts, that the new rates may not reflect the actual cost of delivering care in a sparsely populated rural state — points to the design problem that underlies every state rate decision: no one actually knows what it costs to deliver a unit of ABA therapy in Kearney, Nebraska, and no state has built the cost-accounting infrastructure to find out.
The most sustainable outcomes are in the states that are moving toward credentialing, accreditation, and outcome reporting before they reach for the rate lever. Massachusetts, by implementing an accreditation mandate, is requiring that before Medicaid pays for ABA, the payer can verify that the provider organization meets quality standards that correlate with appropriate clinical practice. It does not solve the volume problem directly, but it creates an infrastructure for distinguishing the clinical outcomes data that would make value-based reimbursement possible.
The structural question — whether $14 billion a year in ABA spending is producing proportionate value for the children and families receiving the services — is one the industry has the data to answer and has not yet answered in the peer-reviewed literature at the scale the problem requires. The spending crisis has created both the political urgency and the policy pressure to force that question into the open. The next chapter of the ABA industry’s relationship with Medicaid will be written by whoever can answer it most credibly.
AT A GLANCE
National ABA Spend: $14.49 billion total Medicaid ABA spending (2024); 279% growth from 2018
ABA Visit Growth: 267% increase in visits (2019–2024); Medicaid +298%, Commercial +249%
Clinician Growth: +135% ABA-related clinicians (2019–2024); Nebraska +761%, Wyoming −32%
Autism Diagnosis Rate: 1 in 31 children (2022) vs. 1 in 150 (2000); 5% Medicaid prevalence vs. 2% commercial
CMS Catalyst: 2014 Informational Bulletin — clarified EPSDT obligation to cover medically necessary ABA; by 2022, all 50 states covered ABA under Medicaid
Reimbursement Model: Fee-for-service, volume-based — incentivizes maximizing billable hours regardless of clinical outcomes (per Trilliant Health)
Indiana: $21M (2017) → $611M (2023) = 2,800% increase; $56M improper payments (HHS OIG, 2019–2020); $78M potentially improper; tiered hour caps under development
Nebraska: $4.6M (2020) → $85M (2024) = 1,700% increase; 48% rate cut for direct therapy (Aug. 2025, from ~$144/hr to $74.80); 51% cut to parent training
North Carolina: $122M (FY2022) → $639M projected (FY2026) = 423% increase; 10% rate cut (Oct. 2025); preliminary injunction by court following lawsuit by 21 families
Arizona: $371M (FY2025), up 43% in one year; Mercy Care, AZ Complete Health, UHC Community Plan contract terminations; Centria lawsuit (Dec. 2025, Maricopa County); class action (Feb. 2026, 11 families)
Colorado: ~$200M+; emergency 20% legislative rate increase (2023); further cuts proposed; Hopebridge exited (2023); provider/parent lawsuit challenging prior authorization
Wisconsin: $18.5M in improper payments (federal audit, 2021–2022); no post-payment reviews conducted since ABA added to Medicaid (2016)
Minnesota: 85 open fraud investigations; FBI raids on ABA providers (2024); criminal investigations ongoing
New York: Proposed 680-hour/year ABA cap (SB S5107); legislation pending; advocacy community mobilized
Federal Pressure: One Big Beautiful Bill Act — $900B+ in Medicaid cuts over 10 years; would shift cost burden to states; per-capita cap or block grant models under discussion
Trilliant Finding: Medicaid autism prevalence (5%) is 2.5x commercial (2%); suggests diagnostic expansion or access-driven utilization gap
Industry Response: Value-based care contracts (Cortica, Hopebridge); outcomes-based research (Action Institute at ABC); legislative advocacy (CASP, state provider coalitions)
Core Policy Tension: Legitimate access expansion vs. volume-driven overutilization vs. inadequate fraud oversight — states using blunt rate cuts instead of targeted utilization management
SOURCES & REFERENCES
Primary Data Source: Trilliant Health, December 2025 analysis of Medicaid & commercial ABA claims data
Federal Reports: HHS Office of Inspector General (Indiana improper payments); CMS 2014 Informational Bulletin (EPSDT)
State Sources: Indiana Family and Social Services Administration; Nebraska DHHS; North Carolina DHHS; Arizona AHCCCS
News Sources: KFF Health News; Stateline (Pew); Behavioral Health Business; Indiana Capital Chronicle; Fortune
Litigation: Centria v. Mercy Care et al. (Maricopa County, Dec. 2025); NC families v. DHHS (Oct. 2025); AZ class action (Feb. 2026)
Legislation: Indiana tiered caps (under development); New York SB S5107 (680 hrs/yr); One Big Beautiful Bill Act (federal)
Published: BreakingNewsABA.com — March 2026