The Retention Numbers
ACROSS THE UNITED STATES — the retention numbers behind ABA therapy are well documented. A 2022 study by Choi and colleagues, published in the Journal of Developmental & Behavioral Pediatrics, examined a random sample of 334 children with autism drawn from 4,145 referrals at a large integrated health system in Southern California between January 2016 and November 2018. Thirteen percent of those referred never received ABA at all. Of the rest, 66 percent were still in services at 12 months. By 24 months, only 46 percent remained, and only 28 percent had received the prescribed service level.
Those figures point to a structural problem. The evidence base for early intensive behavioral intervention recommends 20 to 40 hours per week, often for one to three years, to produce meaningful adaptive behavior gains. When more than half of families disengage before the two-year mark, the clinical promise of the intervention collides with the operational reality of how care is delivered, communicated, and experienced.
The Choi study attributed the discontinuation pattern to factors largely unrelated to clinical progress. Single-parent households were associated with higher discontinuation; children with a prior history of developmental services such as speech therapy or special education were more likely to stay. Workforce churn compounds the picture. CentralReach’s 2025 Autism and IDD Care Market Report put 2024 staff turnover rates in ABA organizations at 77 to 103 percent, with mid-size and enterprise clinics on the higher end.
The opacity that families describe runs through every one of these dynamics. Parents often do not know what happened in a session until days later. They cannot see whether targets are being met or whether the treatment plan is shifting. They are asked to trust a process they cannot observe. The parent portal, once a peripheral feature on most ABA software, has become a central selling point as platforms try to close that gap.
More than half of families leave ABA therapy before the two-year mark. The documented reason is usually not that the therapy stopped working. It is that families lost confidence in a process they could not see.
What the Research Shows
The clinical case for caregiver involvement is not contested. Decades of literature show that parental participation is among the strongest predictors of positive outcomes in early intervention for children with autism. Children spend most of their waking hours outside the therapy room; without caregiver reinforcement, skills learned in structured sessions often fail to generalize. A 1998 study by Ozonoff and Cathcart on a TEACCH-based home program established the early empirical case that parent-led practice in the home produced measurable gains over a four-month period. Subsequent ABA-specific work has reached compatible conclusions across different methodologies.
A 2021 study by Kurzrok, McBride, and Grossman in Autism, drawing on survey data from 438 parents (93 percent mothers) of children with autism aged 2 to 17, examined the relationship between parental intervention involvement, satisfaction with intervention-related training, and autism-specific parental self-efficacy. Parents who reported greater involvement in their child’s treatment had higher self-efficacy regardless of caregiver burden. The intensity of treatment mattered less than the degree to which the parent felt engaged in it. Parental self-efficacy, in turn, has been correlated with reduced parenting stress.
The retention literature reinforces the same pattern from a different angle. Families with more existing infrastructure — a married or partnered second caregiver, prior experience with developmental services, English as a primary language — stay in ABA longer. The Choi sample showed that families who primarily spoke a language other than English were overrepresented in the group that never received ABA at all and underrepresented in the group that stayed at 24 months. The question for the ABA technology industry is whether a well-designed parent portal can replicate some of that scaffolding for families who lack it.
Who Is Building What
Every major ABA software platform has launched, expanded, or repositioned a parent-facing feature in the past two years. Each platform’s approach reflects its design philosophy and target customer.
CentralReach, the category leader by user count with more than 200,000 professionals on the platform, was acquired by Roper Technologies from Insight Partners on March 24, 2025 for a net purchase price of approximately $1.65 billion. The transaction closed in April 2025. CentralReach’s parent portal provides families with session notes, scheduling, and treatment documentation, and supports electronic signatures on session notes. The portal is functional, but provider feedback over time has suggested the parent-facing experience was secondary to the platform’s administrative and billing capabilities, and was designed for compliance workflows rather than progress visibility.
Motivity, NIH SBIR-backed and clinically focused, is the closest competitor on the clinical-data side. Its no-code program builder lets BCBAs create patient-specific protocols, and the platform offers more than 1,000 pre-built program templates with a much larger community library of shared programs. Caregiver data collection is built into the platform: in certain configurations, parents can collect behavioral data directly and have it feed back into the clinical record. The orientation is around the clinical relationship, not the administrative one.
Raven Health, a mobile-first platform designed by a BCBA around field-based therapist workflows, takes a different angle on the parent layer. Its caregiver portal emphasizes plain-language progress narratives over raw clinical data, with AI-generated session summaries and milestone reports designed to be readable without clinical training. Restricted-access scheduling views give caregivers visibility into appointments without exposing protected clinical content.
Ensora Health, the Boston-based KKR portfolio company that rebranded from Therapy Brands on April 7, 2025, markets a parent portal as part of its ABA Suite. The product’s longer-term challenge is integration: because the ABA suite was assembled from separate acquisitions including DataFinch (Catalyst), WebABA, and CodeMetro, the parent experience can vary depending on which combination of modules a practice uses. For multidisciplinary providers that deliver ABA alongside speech or mental health services, a unified cross-disciplinary parent view is the strategic prize, but it remains aspirational.
Rethink Behavioral Health markets a library of more than 1,500 customizable treatment goals with embedded video training, and pushes the parent portal less as a transparency tool and more as a parent-training system. Caregivers watch video demonstrations of techniques and practice them at home; automated progress reports go out on a schedule. Newer entrants are pushing in different directions: Passage Health emphasizes real-time session monitoring; Hi Rasmus emphasizes deep clinical customization; AlohaABA and others compete on simplicity and transparent pricing for small practices where the BCBA-parent relationship is more direct.
The Design Challenge
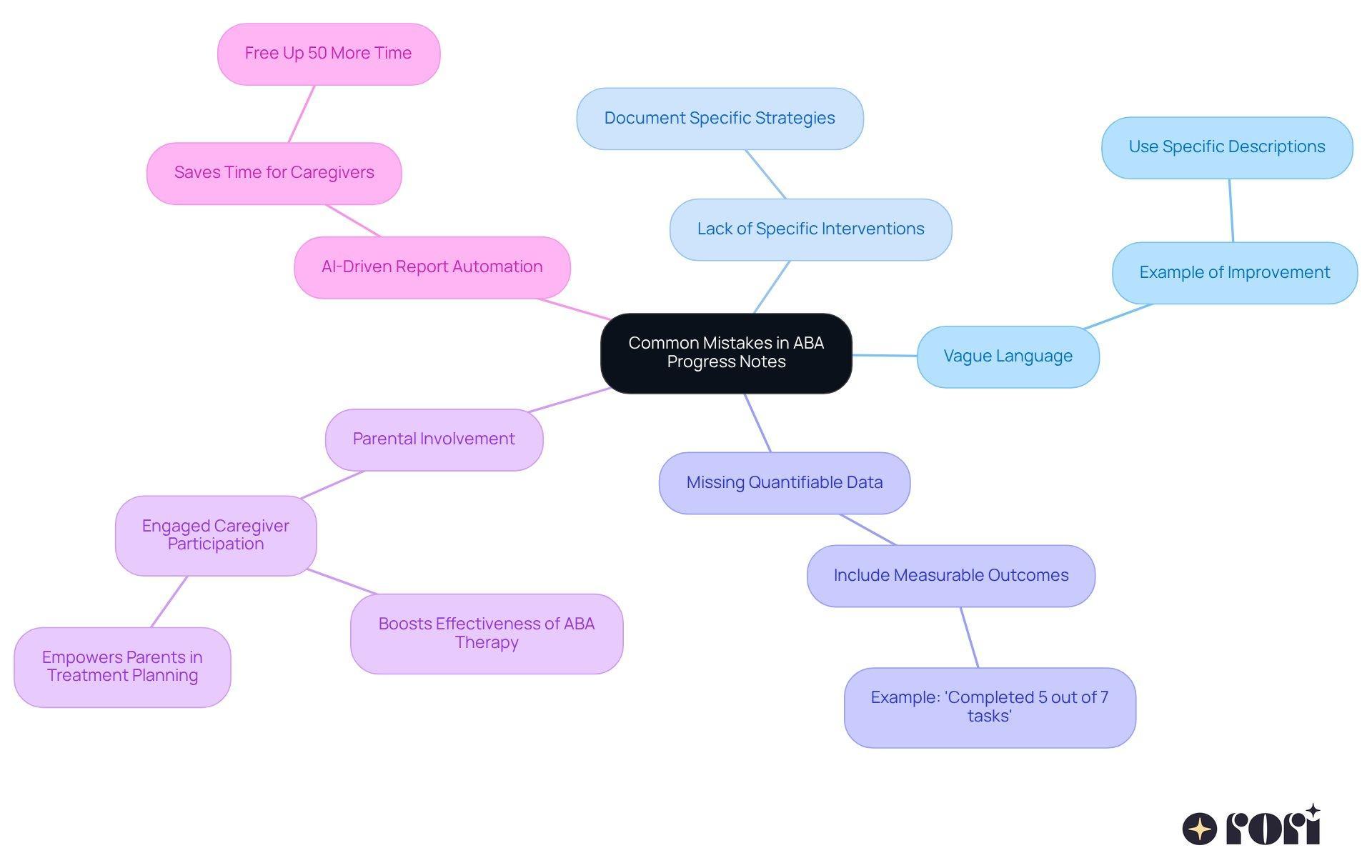
Building a parent portal for ABA goes beyond exposing clinical data to families. ABA data is technical: discrete trial percentages, prompt level hierarchies, behavior reduction graphs, phase change criteria. A parent who logs in and sees a child’s correct response rate drop from 85 percent to 60 percent across a week may experience anxiety, not engagement. Without context, a planned shift from prompted to independent trials, often a sign of progress, looks like regression.
The most effective parent portals mediate clinical data through summary layers: plain-language progress narratives, visual milestone trackers, and contextualized trend explanations. This is where AI is starting to play a real role. Raven Health’s session-summary feature is the clearest example. Instead of a frequency graph with phase change lines, the platform might surface a sentence such as: your child successfully used a greeting with three different people this week, up from one last month. The translation requires both clinical accuracy and communication design, and most platforms are still developing it.
Two-way messaging adds another layer. Parents increasingly expect to message a BCBA through the portal, adding to the BCBA’s administrative burden. A parent message at 9 p.m. that goes 48 hours without a response turns the portal into a source of friction. Privacy compounds the problem. ABA session data contains protected health information, and parent portals need role-based access controls that surface progress and scheduling without exposing internal supervision notes or billing detail. The line between transparency and appropriate professional boundaries is real, and platforms are still feeling out how to draw it without making the experience feel censored.
What’s Missing, and What’s Next
The biggest gaps are structural. Most platforms still treat the parent portal as read-only. Families view data and receive reports, but they cannot contribute structured observations, set their own goals for home practice, or share a digital workspace with the clinical team. Motivity’s caregiver data collection and Rethink’s video training model are the visible exceptions; both are still the minority approach.
Multilingual support is a second gap with direct retention implications. The Choi study showed that non-English-speaking families were overrepresented in non-retention groups. Parent portals available only in English, or with machine-translated content that has not been clinically validated, fail the families most at risk of disengagement. As of early 2026, few ABA platforms market clinically validated multilingual parent interfaces as a standard feature.
Cross-therapy integration is largely absent. Children receiving ABA frequently receive concurrent speech, occupational therapy, and special education services, and parents often log into separate provider portals to track them. The FHIR-based interoperability standards reshaping general healthcare have barely entered the ABA market. Until ABA portals can talk to other therapy platforms and school-based systems, families assemble a complete picture of their child’s progress manually.
For practice owners, the practical implication is direct. The parent portal functions as a retention mechanism as much as a clinical tool, and retention is the operating margin in a field where payer rates are tight and clinician recruitment is expensive. Vendors that answer the parent-experience question well are winning adoption at the practice level even when their enterprise feature sets are thinner than established competitors. The next test for the category is whether AI-generated narratives, bidirectional communication tools, and structured caregiver-led data collection can move the 24-month retention number meaningfully above the current baseline.
AT A GLANCE
| 12-month retention: | ~66% of children referred for ABA remain in services (Choi et al., JDBP 2022, N=334) |
| 24-month retention: | ~46% remain; only 28% receive full prescribed ABA dose (Choi et al., JDBP 2022) |
| Never received ABA: | 13% of referrals never initiated ABA after referral (Choi et al., JDBP 2022) |
| EIBI dose recommendation: | 20-40 hours per week for one to three years; meta-analysis support (Eldevik et al., 2009) |
| Workforce turnover: | 77-103% annual turnover in ABA organizations in 2024 (CentralReach 2025 Market Report); BHCOE median 65% |
| Caregiver self-efficacy: | Greater intervention involvement = higher autism-specific parental self-efficacy regardless of caregiver burden (Kurzrok et al., Autism 2021, N=438) |
| CentralReach (Roper): | Acquired by Roper Technologies for $1.65B net (March 24, 2025; closed April 2025); 200,000+ users; e-signature parent portal |
| Motivity: | NIH SBIR-backed; no-code program builder; 1,000+ templates; caregiver data collection workflow |
| Raven Health: | AI-powered session summaries; mobile-first; plain-language progress narratives for families |
| Ensora Health: | Rebranded from Therapy Brands April 7, 2025 (KKR-owned); ABA Suite parent portal |
| Rethink BH: | 1,500+ customizable treatment goals; video-based parent training; automated progress reports |
| Key gap, language: | Non-English-speaking families overrepresented in non-retention groups (Choi study); few platforms offer validated multilingual interfaces |
| Key gap, interop: | FHIR-based interoperability barely present in ABA market; parents assemble cross-therapy progress views manually |
SOURCES & REFERENCES
| 1. | Choi, K.R., Knight, E.A., Stein, B.D., Coleman, K.J. “Patient Outcomes After Applied Behavior Analysis for Autism Spectrum Disorder.” Journal of Developmental & Behavioral Pediatrics, 43(1):9-16. January 2022. doi:10.1097/DBP.0000000000000995. https://pmc.ncbi.nlm.nih.gov/articles/PMC8702444/ |
| 2. | Kurzrok, J., McBride, E., Grossman, R.B. “Autism-specific parenting self-efficacy: An examination of the role of parent-reported intervention involvement, satisfaction with intervention-related training, and caregiver burden.” Autism. 2021. doi:10.1177/1362361321990931. https://journals.sagepub.com/doi/abs/10.1177/1362361321990931 |
| 3. | Ozonoff, S., Cathcart, K. “Effectiveness of a Home Program Intervention for Young Children with Autism.” Journal of Autism and Developmental Disorders, 28(1):25-32. 1998. doi:10.1023/A:1026006818310. https://link.springer.com/article/10.1023/A:1026006818310 |
| 4. | Eldevik, S., et al. “Meta-Analysis of Early Intensive Behavioral Intervention for Children With Autism.” Journal of Clinical Child & Adolescent Psychology. 2009. doi:10.1080/15374410902851739. |
| 5. | Bennett, A. “Parental Involvement in Early Intervention Programs for Children with Autism.” Master of Social Work clinical research paper, St. Catherine University. 2012. https://sophia.stkate.edu/msw_papers/113/ |
| 6. | Roper Technologies. “Roper Technologies to acquire CentralReach.” News release. March 24, 2025. https://www.ropertech.com/news-releases/news-release-details/roper-technologies-acquire-centralreach |
| 7. | CentralReach. “CentralReach Joins Forces with Roper Technologies.” Company announcement. March 24, 2025. https://centralreach.com/blog/centralreach-joins-forces-with-roper-technologies/ |
| 8. | Larson, C. “Roper Technologies to Buy ABA Software Company CentralReach for $1.65 Billion.” Behavioral Health Business. March 24, 2025. https://bhbusiness.com/2025/03/24/roper-technologies-to-buy-aba-software-company-centralreach-for-1-65-billion/ |
| 9. | CentralReach. “2025 Autism and IDD Care Market Report.” March 2025. https://centralreach.com/resources/autism-idd-care-report/ |
| 10. | Larson, C. “Autism Providers Forecast ‘More Stability in the Workforce’ in 2025.” Behavioral Health Business. February 10, 2025. https://bhbusiness.com/2025/02/10/autism-providers-forecast-more-stability-in-the-workforce-in-2025/ |
| 11. | Ensora Health. “Therapy Brands Is Now Ensora Health.” Press release. April 7, 2025. https://ensorahealth.com/news/therapy-brands-is-now-ensora-health/ |
| 12. | PR Newswire. “Therapy Brands Is Now Ensora Health.” April 7, 2025. https://www.prnewswire.com/news-releases/therapy-brands-is-now-ensora-health-302421655.html |
| 13. | Motivity. Best ABA Practice Management Software [2026]. Product overview. https://www.motivity.net/blog/best-aba-practice-management-software |
| 14. | NIH SEED. Motivity portfolio company profile. https://seed.nih.gov/portfolio/nih-portfolio-company-showcase/motivity |
| 15. | Passage Health. “7 Best ABA Data Collection Software for Clinics in 2026.” January 2026. https://www.passagehealth.com/blog/aba-data-collection-software |
| 16. | Raven Health. ABA software product overview. https://ravenhealth.com/ |
| 17. | Rethink Behavioral Health. Product features and parent training resources. https://www.rethinkbehavioralhealth.com/ |
| 18. | Behavior Frontiers. “Family & Caregiver Involvement in ABA Therapy.” https://www.behaviorfrontiers.com/blog/importance-of-family-and-caregiver-involvement-in-autism-care |
| 19. | BHCOE. “The Role of Caregiver Involvement in ABA Therapy.” Behavioral Health Center of Excellence. July 2021. https://www.bhcoe.org/2021/07/the-role-of-caregiver-involvement-in-aba-therapy/ |
| 20. | BACB. “US Employment Demand for Behavior Analysts: 2010-2024.” 2025. https://www.bacb.com/ |
| 21. | PMC. “Understanding Barriers and Facilitators of Parent/Caregiver Involvement in Home-Based ABA Programming.” 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC12293302/ |