
A scooter, a Duolingo, and a PowerPoint deck
ITAJAÍ, BRAZIL. Augusto was 4 when he was diagnosed with autism, level 2 support. He is 8 now, and on most days reads as level 1. The years between are why his parents, Aline Bernardi and Diogo Ruiz, built Mirimim.
The defining moment was not the diagnosis. It was a scooter. Augusto, by his parents’ account, would see another child on a scooter and run at it. Sometimes he took it. Sometimes he scared the child. He was not aggressive. He simply did not have the social script for asking, waiting, and accepting the answer. Therapy hours alone were not closing that gap, because therapy ended and the rest of the day did not.
The fix started on a family trip to Spain. Bernardi, an environmental engineer who had spent her career in project work at a multinational, wanted Augusto to pick up a few words of Spanish. She put Duolingo on his tablet. He engaged. He repeated. He learned. Bernardi and Ruiz, an entrepreneur and Augusto’s stepfather, asked the question that became the company: if a gamified loop could move a child through a foreign language, could the same loop move a child through the social scripts that therapy was teaching one hour at a time?
The first version was built in PowerPoint. They translated two evidence-based behavioral techniques, choices and consequences and visual empathy, into clickable scenarios. They tested the scenarios on Augusto. After enough repetitions, he walked up to another child at a park and asked to borrow a scooter. The child said yes. The app, by Bernardi’s telling, was built around that one outcome.
“What if we could apply that same model to social skills?” -Aline Bernardi, co-founder and CEO, Mirimim (2025)
Therapists who saw the prototype asked for more content. The PowerPoint became an app. The app launched in May 2025. Eleven months later, by the company’s count, more than 17,000 children had used it, more than 1,300 professionals had adopted it in clinical practice, and it was running in roughly 500 institutions across 21 of Brazil’s 27 states. None of that came from paid marketing.
A complement to ABA, not a competitor
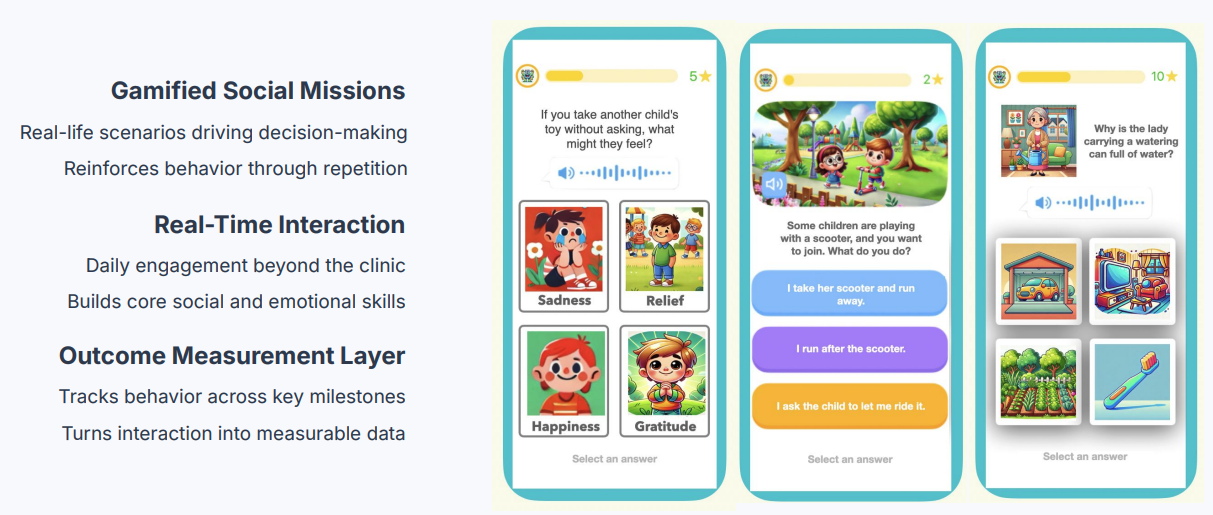
Mirimim is not an ABA platform. It does not employ BCBAs, deliver one-on-one therapy, or bill insurance for sessions. What it does is digitize protocol-style activities (choices and consequences, active listening, logical sequencing) into short interactive missions a child completes between therapy hours. The company describes its first feature as a Duolingo for social and emotional skills.
The behavioral-tech category Mirimim sits in is real but thin. Floreo, the U.S. virtual-reality platform for autism therapy, has built around immersive in-session content and is reimbursed in some Medicaid programs. Cogniable, out of India, sells an ML-based detection and recommendation tool for clinics. Social Cipher, a Los Angeles game studio, builds narrative video games tied to social-emotional curricula. Each is a point tool. None has positioned itself as the connective tissue between the clinic and the home in the way Mirimim describes its product.
Bernardi and Ruiz were selected for the 2026 cohort of the Multiple accelerator, the California-based 501(c)(3) autism-tech program founded by Dan Feshbach, who previously co-founded the special-education platform TeachTown. Multiple’s portfolio includes Floreo, Social Cipher, Cogniable, and several other companies operating at the intersection of autism and consumer technology. Mirimim’s pitch within that group is structural rather than clinical: the company is selling itself as the layer that turns at-home activity into auditable data, not as a new modality of therapy.
That positioning matters because the U.S. autism-care market is shifting around it. Florida moved its ABA claims into Managed Care Organizations in 2025. Indiana adopted a tiered system that narrows full benefits to its highest-need families. The Autism CARES Act reauthorization, signed in December 2024, runs $1.95 billion through fiscal year 2029, and the practical effect is that payers, both Medicaid and private, are looking for tools that produce measurable outcomes rather than units of service. The data-layer pitch is a response to that pressure.
The supply problem the whole industry is fighting
The conditions Mirimim is responding to are the same ones every operator in the category is dealing with. The U.S. ABA market was valued at roughly $7.97 billion in 2025 and is projected to reach $9.96 billion by 2030, a compound annual growth rate of about 4.56%. Behind the dollars is a workforce gap. There were roughly 75,600 active Board Certified Behavior Analysts in the United States as of mid-2025, against more than 103,000 open BCBA-level postings at the end of 2024. Smaller centers report annual turnover near 80%. Burnout surveys put roughly 93% of behavioral-health workers somewhere on the spectrum from mild to severe.
Demand is moving the other way. The CDC’s ADDM Network now estimates 1 in 31 children is diagnosed with autism spectrum disorder, up from 1 in 36 in the prior cycle. Brazil does not publish a comparable national figure, but the country’s autism advocacy infrastructure (the APAEs, the AMAs, the Casa do Autista network) reports the same demand pattern. Families with autistic children regularly leave the workforce. The Sparks for Autism initiative places the share of mothers who leave their jobs to provide care at 43% in Brazil. Annual therapy costs, in research summaries from the University of São Paulo and the FIPE foundation, can exceed R$100,000.
What Mirimim sells against this backdrop is engagement that costs nothing per minute. A child practices a social script on a tablet at home; a therapist reviews the resulting interaction data in the next session; a payer sees usage frequency and progression as evidence of adherence. The company says professionals report a 100% intent-to-continue rate after using the platform clinically, and 92% rate the platform as highly relevant for social-skills development. Those are self-reported figures from the company’s own surveys of its therapist users, not from independent research.
What sets the model apart, by Bernardi’s telling
Three operational features are the spine of Mirimim’s pitch to professionals and institutions. The company describes each in its sales materials and in interviews with Brazilian trade press.
A protocol-derived activity library. The content is not generic SEL curriculum. The activities are translations of specific behavioral-development techniques (visual empathy, choices and consequences, logical sequencing, active listening) into short scenarios a child completes in two-to-five-minute sessions. The company points to literature from Cambridge, Harvard, and Yale on each technique’s use with autistic children. It does not claim that Mirimim itself has been the subject of a randomized trial. It claims that the underlying methods have.
A family-first deployment. Most autism digital tools are sold into clinics. Mirimim’s organic growth came the other way around. Parents downloaded it, used it at home with their child, and then handed the phone to their therapist at the next session. The therapist asked what the app was, downloaded it, and started recommending it. By the time the founders started thinking institutionally, the company was already inside about 500 Brazilian organizations.
A data layer aimed at operators, not patients. The product roadmap is to evolve from content-led to data-led. Each session captures interaction data: response patterns, latency, repetition, choice consistency. The company says the next version will use those signals to tune difficulty per child and surface patterns to clinicians. The thesis is that, in a value-based-care world, the operator that sees what happens between sessions has a structural advantage over the operator that does not.
What Mirimim does not claim. Mirimim does not present itself as ABA. It does not claim to replace one-on-one therapy. It does not market FDA clearance, which it does not have. It is not a digital therapeutic in the prescription sense. The clinical evidence base for the platform itself is, by the company’s own admission, early. What is being measured at scale is engagement and adherence; what is not yet being measured at scale is durable behavioral change attributable to the app rather than to the therapy it sits alongside. This is a real gap, and it is the question the company’s next phase has to answer.
In a value-based-care world, the operator that sees what happens between sessions has a structural advantage over the operator that does not. Whether Mirimim’s data layer is the one operators choose is the open question its institutional pilots will answer.
The next decade
The forward bet is institutional. The most concrete signal is a proposal in front of Dr. Sulaiman Al Habib Medical Group, the largest private healthcare provider in the Middle East, with 20-plus facilities across Saudi Arabia, the UAE, and Bahrain and roughly $3.65 billion in trailing 12-month revenue as of December 2025. The proposal, dated this year, lays out a six-month proof of concept covering 100 children inside the group’s TEAbraça autism program. The deliverables include onboarding, monthly engagement reports, behavioral-pattern analysis, and a consolidated outcomes file at the end. The company is positioning the engagement as a tool for clinical auditing inside an outcome-based program, not as a marketing pilot.
Domestic validation is broader. Mirimim sits inside the BNDES Garagem 2025 acceleration cohort, the Brazilian national-development bank’s impact-business program. The Federal University of Paraná’s graduate program at the Hospital de Clínicas selected the platform as a research subject. The Paraná State Legislative Assembly recognized Bernardi for the work this year. The company has been included in an early evaluation phase of the Instituto Jô Clemente’s Prêmio Dona Jô Clemente, the inclusive-education research prize launched in late 2025.
The U.S. opening is real but unproven. The company lists its corporate base as San Francisco; its founders still operate from Itajaí, where Augusto goes to school. The Multiple Hub seat puts Bernardi and Ruiz in front of U.S. payers, autism-tech investors, and operators who can route the product into clinical pipelines. None of that converts to revenue automatically. The U.S. behavioral-health market is harder to penetrate than the Brazilian one because the gatekeepers are harder. Insurance contracting, FDA pathways for digital therapeutics, state Medicaid carve-ins, and the fragmented BCBA-led practice landscape all sit between an organically grown Brazilian app and a reimbursable U.S. intervention.
The open questions are specific. Will the Saudi proof of concept produce data clean enough to support an outcomes-based contract, or will it surface engagement without behavioral transfer? Will an independent clinical study materialize, and will it survive peer review? Will Mirimim’s organic-growth playbook hold inside U.S. clinical operations, where competing point tools have spent years and capital trying to crack the same channels? And will the founders, who have been the company’s product team, sales team, and clinical-partnerships team, build the operating bench needed to answer all three at once?
The Brazilian proof is in. The company reached 17,000 children without an ad budget. The international proof is what the next 24 months are about. If the data layer works, Mirimim becomes one of the first non-U.S.-built autism-tech companies to land inside a value-based-care contract at scale. If it does not, the company stays a strong Brazilian consumer product. The bet is that the operators who decide first are the ones who already feel the supply problem most acutely.
| Founders: | Aline Bernardi (CEO) and Diogo Ruiz (co-founder) |
| Company founded: | 2025 (app launch May 2025); prototype built 2024 |
| Headquarters: | San Francisco, CA (corporate); founders operate from Itajaí, Brazil |
| Origin: | Built around founders’ son Augusto, diagnosed with ASD level 2 at age 4 |
| Children reached: | 17,000+ (company-reported, April 2026) |
| Professional users: | 1,300+ across roughly 500 institutions, 21 of 27 Brazilian states |
| Self-reported metrics: | 100% intent-to-continue from professional users; 92% rate platform highly relevant |
| Self-reported ROI claim: | $4 to $6 saved per $1 invested (company materials; not independently verified) |
| Revenue model: | Enterprise/government licensing ($200K to $10M annually); SaaS at $20 to $50 per patient per month (company-stated) |
| Most concrete institutional pilot: | Six-month proof of concept proposal with Dr. Sulaiman Al Habib Medical Group, 100 children |
| Accelerator: | Multiple Hub (California, 2026 cohort); BNDES Garagem 2025 (Brazil) |
| U.S. ABA market context: | $7.97B (2025); ~$9.96B projected by 2030; 75,600 active BCBAs vs. 103,000+ open postings |
SOURCES & REFERENCES
| 1. | Mirimim. Submission to BreakingNewsABA, including company materials, founder bios, and Dr. Sulaiman Al Habib proposal document. April 2026. |
| 2. | Bernardi A. LinkedIn profile. Retrieved April 2026. https://br.linkedin.com/in/alinebernardi/en |
| 3. | Mirimim. Company website. Retrieved April 2026. https://www.mirimim.com |
| 4. | Zigart AC. “Família de Itajaí desenvolve app que ajuda crianças autistas a desenvolver habilidades.” Diarinho. April 2025. https://diarinho.net |
| 5. | Canal Autismo. “Aplicativo Mirimim amplia alcance e é reconhecido em evento estadual de inclusão no PR.” June 2025. https://www.canalautismo.com.br |
| 6. | Gazz Conecta. “Aplicativo Mirimim ajuda na socialização de crianças com autismo.” 2025. https://gazzconecta.com.br |
| 7. | Multiple Hub. Accelerator program and team pages. Retrieved April 2026. https://www.multiplehub.org |
| 8. | Dr. Sulaiman Al Habib Medical Services Group. Investor relations and financial disclosures via Saudi Exchange (Tadawul: 4013). Retrieved April 2026. https://hmg.com |
| 9. | PitchBook. Dr Sulaiman Al Habib company profile. Retrieved April 2026. https://pitchbook.com/profiles/company/433337-41 |
| 10. | BNDES. “BNDES Garagem anuncia as 100 startups selecionadas para a aceleração em 2025.” November 17, 2025. https://agenciadenoticias.bndes.gov.br |
| 11. | Centers for Disease Control and Prevention. ADDM Network autism prevalence reports. 2024-2025 release. |
| 12. | Public Law 118-194. Autism CARES Act of 2024 reauthorization. December 2024. |
| 13. | Behavior Analyst Certification Board. Certificant data summaries. Mid-2025. |
| 14. | Global Market Insights and related industry research firms. U.S. ABA market sizing (2025-2030 projections). Trade publication summaries, 2025-2026. |









