The Biggest Payer in the Room
MINNETONKA, MINNESOTA – UnitedHealth Group is not just the largest health insurer in the United States. It is the largest healthcare company in the world by revenue, ranked seventh on the Fortune Global 500. In 2024, the company reported $400.3 billion in revenue and served 50.7 million medical members domestically. In 2025, revenues grew to nearly $448 billion. The company’s insurance arm, UnitedHealthcare, covers approximately 8.4 million Medicare Advantage members, 7.4 million Medicaid members, and tens of millions of commercially insured individuals through employer-sponsored and individual plans. It operates in every state.
Behavioral health benefits for UnitedHealthcare members are managed by Optum, a subsidiary that has grown into one of the most powerful entities in American healthcare. Optum processes prior authorization requests, conducts clinical reviews, manages provider networks, and makes the medical necessity determinations that decide whether a child with autism will receive the ABA therapy hours their BCBA has recommended. For the approximately 10,000 children with autism receiving ABA through UnitedHealthcare’s Medicaid plans alone — and thousands more on commercial plans — Optum is the gatekeeper.
The company’s scale gives it extraordinary leverage. When UnitedHealthcare sets a reimbursement rate, it shapes the market. When Optum tightens its authorization criteria, providers across dozens of states feel the effect simultaneously. When the company decides to contract its ABA network, hundreds of families can lose access to their provider in a single administrative action. No other payer in the ABA industry has this combination of size, vertical integration, and decision-making centralization. And no other payer has had its internal ABA strategy laid bare in the way UnitedHealthcare’s was in December 2024.
The Playbook: What the Leaked Documents Revealed

In December 2024, ProPublica published an investigation based on leaked internal Optum documents that detailed the company’s strategic approach to managing its ABA therapy costs. The documents, which ProPublica described as the company’s internal playbook, revealed a multifaceted cost-containment campaign targeting ABA services across the company’s Medicaid plans.
The strategy had several components. First, Optum was implementing what the documents called “rigorous utilization management,” which involved scrutinizing individual patients’ therapy hours through clinical reviews that could result in denials or reductions. The internal records explicitly described an “approach to authorizing less units than requested” — language that suggests a systematic practice of approving fewer hours than BCBAs and clinical teams determine to be medically necessary.
Second, the company was contracting its ABA provider networks within Medicaid plans. Internal documents showed that in some states, Optum planned to remove more than 40 percent of in-network ABA provider groups. The documents also indicated that as many as 19 percent of current ABA clients could see their authorized hours reduced or eliminated entirely as a result of these strategies.
Third, Optum was targeting providers for scrutiny based on what the documents described as “outlier patterns.” Providers could be flagged for billing on weekends or holidays, serving multiple family members, having long clinician or patient days, providing what Optum characterized as “above average delivery” of services, or showing sudden changes in patient volume or claims. ABA providers told ProPublica that many of these patterns are inherent to the delivery model of ABA therapy — intensive, daily, often involving siblings, and routinely requiring weekend hours to accommodate school schedules.
Perhaps most striking was the internal contradiction at the heart of the strategy. The leaked documents acknowledged that ABA is the “evidence-based gold standard treatment for those with medically necessary needs.” The company’s own Medicaid ABA spending had grown approximately $75 million year-over-year, driven by a 20 percent increase in the number of Medicaid patients accessing therapy. Rather than treating the increase as an indicator of growing need, the documents framed it as a cost problem requiring containment.
“They’re denying access to treatment and shrinking a network at a time when they clearly know that there is an urgent need.” — Karen Fessel, Mental Health and Autism Insurance Project
UnitedHealthcare and Optum declined ProPublica’s request for an on-the-record interview about the story, citing the December 4, 2024 killing of UnitedHealthcare CEO Brian Thompson as the reason they could not engage with the reporting.
The Capitation Incentive: Why Managed Care Rewards Denial
To understand why UnitedHealthcare’s internal strategy targets ABA costs so aggressively, it is necessary to understand how Medicaid managed care financing works. In most states where UnitedHealthcare administers Medicaid benefits, the state pays the company a fixed per-member-per-month capitation rate. This rate is calculated to cover the expected cost of all services for that member over the contract period. If UnitedHealthcare spends less than the capitation amount on actual care, it keeps some or all of the difference as profit. If it spends more, it absorbs the loss.
This structure creates a direct financial incentive to reduce the cost of care delivered. Every ABA hour that is not authorized is money that remains with the managed care organization. Every provider that is removed from the network reduces the pool of clinicians who can generate claims. Every reauthorization that results in a reduction from 30 hours per week to 20 hours per week saves the company roughly $500 to $1,000 per week per child, depending on the rate. Multiply that by thousands of children across two dozen states and the savings are significant.
Federal regulators and experts have acknowledged that capitation-based managed care creates this incentive. ProPublica’s reporting cited it explicitly: states pay private insurers a fixed amount per patient, regardless of the frequency or intensity of services used, and when companies spend less than the allotted payment, they are typically allowed to keep some or all of what remains. The incentive structure does not make cost containment inherently improper — managed care is designed to encourage efficiency. But when cost containment takes the form of systematically authorizing fewer hours than clinicians recommend for children with autism, the line between efficiency and denial of medically necessary care becomes the central question.
State-by-State: Where the Network Is Shrinking
The leaked Optum documents identified specific states where the company was focusing its ABA cost-containment efforts: Arizona, Nebraska, Tennessee, Virginia, New Jersey, Indiana, and Louisiana. These were the states whose Medicaid plans yielded the highest ABA costs for the company. The strategy was not uniform — each state had different network dynamics and regulatory environments — but the direction was consistent: fewer providers, more scrutiny, lower authorized hours.
Louisiana provides the most detailed case study. Internal documents showed Optum planned to exclude approximately 40 percent of in-network ABA provider groups in the state and estimated that about one in five children whose ABA treatment was covered by UnitedHealthcare’s Medicaid plan could lose access to care. The Aspire Behavioral Health Center in Lafayette, which serves approximately 160 patients with Medicaid coverage, was subjected to both a payment integrity audit and an in-person quality review. Its founder, psychologist Joslyn McCoy, reported that despite passing the reviews, Optum continued to challenge individual patient authorizations. Her center maintained a waitlist of approximately 260 children.
The Louisiana situation reached a further inflection point in December 2025, when the Louisiana Department of Health announced it would not renew its Medicaid managed care contract with UnitedHealthcare beyond the end of 2025. A 90-day extension through March 31, 2026 was negotiated to avoid abrupt disruption for the approximately 330,000 Medicaid enrollees in UnitedHealthcare’s plan. The decision came amid allegations that UnitedHealthcare had violated its state contract by withholding documents related to prescription drug pricing, and a separate lawsuit by then-Attorney General Liz Murrill alleging OptumRx had overcharged the state’s Medicaid program. By April 2026, all UnitedHealthcare Medicaid members in Louisiana will be reassigned to the state’s five remaining managed care organizations.
In Arizona, Optum’s network contraction overlapped with broader Medicaid ABA access problems. The state’s Mercy Care MCO — which is not affiliated with UnitedHealthcare but operates in the same market — imposed a combined 40 percent rate reduction and terminated contracts with the two largest ABA providers in 2025, leaving approximately 1,000 families without covered providers. UnitedHealthcare’s simultaneous network tightening in the state compounded an already critical access crisis.
Optum’s own provider network page confirms that its Medicaid ABA network is selectively restricted. As of 2026, Optum states that it is only accepting new Medicaid network participation requests for ABA and BCBA providers “in areas where we have a network need.” Its commercial and Medicare Advantage networks, by contrast, remain open to all types of behavioral health providers. The differential treatment of Medicaid ABA networks — the very population with the strongest federal coverage protections under EPSDT — is precisely the pattern that the leaked documents described.
What BCBAs Experience: The View from the Front Lines
For Board Certified Behavior Analysts working with UnitedHealthcare and Optum plans, the prior authorization process is the defining administrative challenge of their practice. Every authorization request begins with the same basic requirements: a documented autism spectrum disorder diagnosis, a comprehensive treatment plan with measurable goals, and clinical justification for the number of hours requested. What varies — and what providers describe as opaque, inconsistent, and increasingly adversarial — is what happens after submission.
Optum uses what providers describe as a “two-key” system for initiating ABA services. The first authorization covers the initial assessment, typically 10 to 15 hours, during which a BCBA evaluates the child and develops a treatment plan. The second authorization covers the treatment itself, with Optum reviewing the plan and determining how many hours per week it will approve. It is at this second step that the friction intensifies.
BCBAs across the country report a recurring pattern: they submit a treatment plan recommending a specific number of hours based on their clinical assessment, and Optum approves fewer hours than requested without providing a transparent clinical rationale for the reduction. A BCBA might recommend 30 hours per week of direct therapy for a child with significant behavioral challenges, only to have Optum authorize 20 or 25. The reduction may not come with a detailed explanation of which clinical criteria were not met. It arrives as an authorization with a lower number.
The reauthorization cycle compounds the problem. ABA authorizations are typically issued for periods of several months. At each renewal, the provider must submit updated progress data, demonstrate measurable gains, and justify continued treatment at the requested intensity. Providers describe a dynamic in which Optum reviewers scrutinize data for evidence that the child is improving — and use that improvement as justification for reducing hours, on the theory that the child is progressing and therefore needs less. But if the child is not improving, Optum may use that as evidence that the treatment is not effective and should also be reduced. The provider is caught in a clinical catch-22: progress and lack of progress both become grounds for cutting hours.
The case that crystallized the ProPublica investigation involved a Louisiana child named Benji, whose clinical team requested an increase in his therapy hours after he experienced behavioral regression. Optum denied the request, stating that the child had been in therapy for too long and was not showing enough progress to ultimately graduate from ABA. Experts consulted by ProPublica said the denial reflected a fundamental misunderstanding of autism and ABA therapy: that it should be treated like an acute intervention with a defined endpoint rather than an ongoing support that may be needed for years or indefinitely. Professional guidelines for ABA treatment, which Optum’s own clinical criteria reference, state that there is no specific limit on the duration of a course of treatment.
When Benji’s clinical team conducted a reversal-to-baseline experiment — temporarily withdrawing the behavioral interventions to document what happened without them — the results were dramatic. The team documented the behavioral deterioration with data and photographs of staff injuries. They faxed the evidence to Optum requesting reconsideration. The insurer did not change its decision. Benji’s mother was left to pursue an administrative law review to attempt to overturn the denial.
“Challenges that often come with autism shouldn’t be looked at like an injury that you’re going to get better from quickly and then the treatment can stop. Treatment may still be medically necessary even if it’s for skill maintenance or the prevention of regression.” — Christa Stevens, Autism Speaks
The administrative burden extends beyond individual denials. ABA providers working with Optum report that the prior authorization process consumes significant clinical and administrative hours — time spent preparing documentation, responding to reviewer questions, submitting appeals, and managing the uncertainty of whether authorized hours will be maintained at the next reauthorization. For small and mid-sized practices, this burden can be existential. As one provider told ProPublica: when denials become routine, clinicians are disincentivized from working with insurance companies at all, and private practices that rely on insured patients may eventually close.
The Hidden Barrier: Medically Unlikely Edits and Claims Denials
Beyond the prior authorization process, ABA providers working with UnitedHealthcare and other payers face an additional layer of claims-level restrictions through the application of Medically Unlikely Edits. MUEs were established by CMS to flag potential fraud and billing errors by identifying the maximum number of units a provider would typically report for a specific CPT code in a single day. They were designed as fraud-detection tools, not as limits on medically necessary treatment. CMS has stated explicitly that claims exceeding MUE thresholds can be paid if the services were actually provided, properly documented, and medically necessary.
In practice, however, many payers — including UnitedHealthcare and its affiliated plans — apply MUEs as de facto daily caps on ABA services. When a provider submits a claim for a day of comprehensive ABA treatment that exceeds the MUE threshold for a given code, the claim may be partially or fully denied. The ABA Coding Coalition and the Council of Autism Service Providers have both documented this pattern and urged payers to adopt the more permissive Medicaid MUE values rather than the more restrictive Medicare values, which were not designed for the intensive treatment patterns typical of ABA therapy for children with autism.
The practical effect is significant. A child receiving 30 or more hours per week of direct therapy may generate daily unit counts that exceed MUE thresholds for codes like 97153. When the claim is denied at the MUE level, the provider must appeal — a process that requires detailed documentation demonstrating that the services were medically necessary and actually delivered. The burden of proof is high, and the appeal process is time-consuming. Some providers report adjusting their billing practices to stay within MUE thresholds, effectively limiting the hours they deliver or splitting sessions across multiple days to avoid denials. This practice, which the ABA Coding Coalition has warned against, results in underbilling for services actually rendered and can increase cost-sharing for families through additional copays.
CASP has urged providers to continue billing for all medically necessary services, including those that exceed MUEs, and to appeal every denial. The rationale is that MUE thresholds are determined in part by what claims data shows as customary. If providers systematically underbill, the data will continue to support restrictive thresholds, and the cycle will perpetuate. The coalition is also working directly with CMS to increase Medicare MUE values for ABA codes to better reflect actual clinical practice.
What the Payer Says Publicly: Commitments, Criteria, and Contradictions
UnitedHealthcare’s public-facing position on ABA therapy is unambiguous: it covers ABA as a medically necessary treatment for autism spectrum disorder, consistent with state mandates, federal Medicaid requirements, and the Mental Health Parity and Addiction Equity Act. The company’s published clinical guidelines, managed through Optum, reference the Council of Autism Service Providers practice guidelines and require that ABA services be supervised by a licensed BCBA, that treatment plans include measurable goals, and that medical necessity be documented at each authorization period.
Publicly, UnitedHealthcare has also positioned itself as a leader in prior authorization reform. In June 2025, the company was among more than 50 major insurers that pledged to streamline prior authorization, reduce the number of services requiring approval, and ensure that all denials based on medical necessity would be reviewed by a licensed clinician. The commitments, made in partnership with CMS, included a promise to reduce prior authorization requirements for certain claims by January 1, 2026. The company had previously announced a 10 percent reduction in prior authorization requirements for 2025, following a 20 percent reduction in 2023 and the introduction of a Gold Card program in 2024 that allows some providers to bypass prior authorization entirely.
The contradiction between these public commitments and the internal playbook revealed by ProPublica is the core tension of the UnitedHealthcare ABA story. The company publicly pledges to reduce administrative barriers. Internally, it develops strategies to authorize fewer units than requested, flag providers for delivering above-average services, and shrink networks in states where Medicaid ABA costs are growing. The question is which version of UnitedHealthcare’s policy families and providers actually encounter.
The data suggests the answer. UnitedHealthcare’s Medicare Advantage prior authorization denial rate in 2023 was 9.1 percent, above the industry average. The company’s appeal overturn rate was 85.2 percent, meaning the vast majority of denials that were challenged were reversed — an indicator that many initial denials may not have been clinically justified. For ABA providers, the denial-and-appeal cycle is not an occasional inconvenience. It is a structural feature of the authorization process that consumes administrative hours, delays patient care, and creates uncertainty for families whose children’s therapy can be interrupted at any reauthorization point.
The Parity Question: Is UnitedHealthcare Treating ABA Differently?
 parity violations and secured a landmark $15.6 million settlement in 2021. | Photo: Wikimedia Commons” />
parity violations and secured a landmark $15.6 million settlement in 2021. | Photo: Wikimedia Commons” />The Mental Health Parity and Addiction Equity Act of 2008 requires that insurers apply the same standards to mental health and substance use disorder benefits as they do to medical and surgical benefits. If an insurer does not require prior authorization for comparable medical treatments, it cannot require prior authorization for behavioral health treatments. If it applies less restrictive review criteria to physical health services, it must apply equally permissive criteria to mental health services. The law is designed to prevent exactly the kind of differential treatment that ABA providers describe experiencing with UnitedHealthcare and Optum.
UnitedHealthcare has a documented history of parity violations. In 2021, the company paid $15.6 million to settle federal and state investigations alleging that it violated parity laws by improperly restricting coverage of outpatient psychotherapy. The New York Attorney General’s office found that the company had denied coverage to more than 20,000 New Yorkers for mental health and substance abuse treatment. In 2025, Delaware issued $450,000 in mental health parity penalties against UnitedHealthcare. The landmark Wit v. United Behavioral Health case found that UBH — operating as Optum — had created defective medical review criteria that wrongly rejected coverage for more than 50,000 individuals seeking behavioral health treatment, systematically favoring acute, short-term care over the chronic and ongoing treatment that conditions like autism require.
Whether UnitedHealthcare’s ABA authorization practices specifically violate parity law is a question that advocates and legal experts have raised but that has not been definitively resolved through litigation focused exclusively on ABA. The argument is straightforward: if Optum applies utilization management criteria to ABA therapy that are more restrictive than what it applies to comparable medical treatments — such as physical therapy or oncology — then it is violating parity. If the company’s internal strategy to authorize fewer hours than requested for ABA has no equivalent in its management of medical benefits, the differential treatment may be illegal.
A class-action complaint filed by Psych-Appeal against United Behavioral Health specifically alleged that UBH’s denial of ABA therapy for a teenager with autism violated the parity act. The case argued that the company’s medical review criteria were structured to deny ongoing, intensive behavioral health treatments in favor of short-term interventions — a pattern that, if applied to ABA, would systematically underauthorize the hours that children with autism need.
The Bigger Picture: UnitedHealth Under Scrutiny
The ABA authorization strategy revealed by ProPublica exists within a broader context of intensifying scrutiny of UnitedHealth Group. In 2025, the Department of Justice opened both criminal and civil investigations into the company’s Medicare billing practices, focusing on whether UnitedHealthcare inflated risk-adjustment scores to increase federal payments to its Medicare Advantage plans. The company confirmed the investigation in July 2025 and said it was cooperating with the DOJ’s requests. The probe subsequently expanded to encompass billing practices at Optum Rx and physician reimbursement practices. The Wall Street Journal reported that DOJ investigators interviewed former UnitedHealth-employed clinicians who described feeling pressured to add diagnoses that increased payments, and that the FBI and HHS Office of Inspector General were involved.
Separately, the company faced lawsuits alleging that an AI-driven tool developed by its subsidiary NaviHealth (later rebranded Optum Home & Community Care) was used to prematurely deny skilled nursing care to Medicare Advantage members. The lawsuit, originally filed in 2023, alleged that the nH Predict tool overrode physicians’ clinical decisions. A federal judge ordered UnitedHealth to produce discovery documents in the case in March 2026.
The December 2024 killing of UnitedHealthcare CEO Brian Thompson outside a New York City investor conference became a lightning rod for public anger about insurance denials and the perceived gap between the industry’s profits and patients’ access to care. UnitedHealth Group’s stock fell more than 42 percent in 2025. CEO Andrew Witty resigned abruptly in May 2025 after the company suspended its financial guidance amid surging medical costs. Former CEO Stephen Hemsley returned to lead the company.
For ABA providers and families, the question is whether the company’s current period of corporate crisis and regulatory scrutiny will translate into any change in how it manages ABA authorizations. The structural incentives remain the same: Medicaid ABA costs are growing, the number of children diagnosed with autism continues to rise, and the company’s strategy documents explicitly frame these trends as cost problems rather than indicators of unmet need. Until the incentives change — through litigation, regulation, or legislative action — providers and families should expect the playbook to remain in effect.
“If these kids get the intervention they need as children, then there will be tremendous cost savings over the course of their lives.” — Lorri Unumb, CEO, Council of Autism Service Providers
What Families and Providers Need to Know
For families navigating UnitedHealthcare and Optum for ABA services, documentation is the single most important tool. Every authorization request should include a detailed treatment plan with measurable goals, progress data from the current authorization period, standardized assessment results, and a clear clinical justification for the number of hours requested. If Optum reduces authorized hours, request a written explanation of the specific clinical criteria that were not met.
If a prior authorization is denied or reduced, you have the right to appeal. For commercial plans, the appeal deadline is typically 180 days from the denial. For Medicare Advantage plans, it is 65 days. Appeals should include updated clinical documentation, letters of medical necessity from the treating BCBA and referring physician, and reference to the professional treatment guidelines that support the requested intensity. The CASP practice guidelines, which Optum’s own criteria reference, state that there is no specific limit on the duration of ABA treatment.
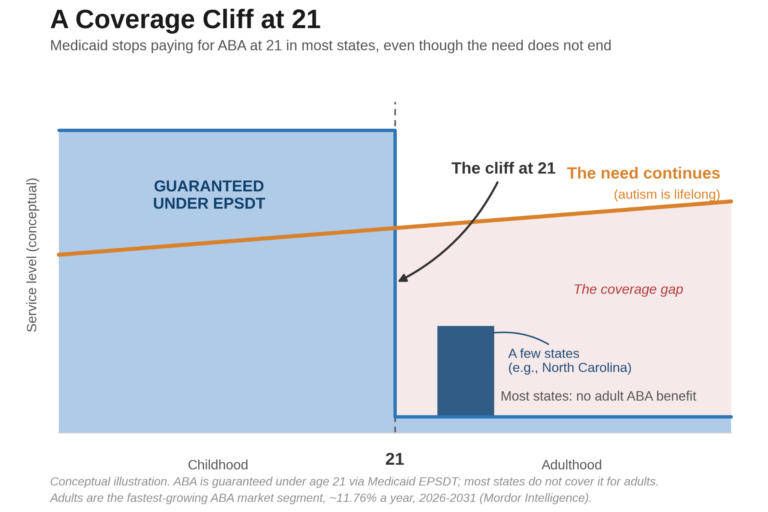
For Medicaid members, EPSDT protections apply to all children under 21. UnitedHealthcare, as a Medicaid managed care organization, is legally required to cover all medically necessary ABA services for Medicaid-eligible children. Hard caps on hours that override a physician’s determination of medical necessity are not permitted under EPSDT. If Optum denies or reduces services for a Medicaid-covered child, the family has the right to request a Medicaid fair hearing and can request that services continue during the appeal under “aid pending.”
For providers, maintaining detailed clinical records, using standardized assessments, and documenting the functional impact of any hour reduction are essential both for the authorization process and for any potential legal action. If Optum’s authorization practices appear to violate mental health parity requirements — for example, if the company applies prior authorization to ABA but not to comparable medical treatments — providers and families can file complaints with their state insurance commissioner and with the U.S. Department of Labor’s Employee Benefits Security Administration.
The mandate exists. The parity law exists. The appeals process exists. The problem is that the people responsible for honoring these protections have, in too many cases, built a system that treats their violation as a cost-saving strategy. The families and providers on the other side of that system cannot afford to wait for the system to fix itself.
AT A GLANCE
Company: UnitedHealth Group (NYSE: UNH); insurance arm: UnitedHealthcare; behavioral health managed by Optum
Scale: 50+ million domestic medical members; nearly $448 billion in 2025 revenue; Medicaid plans in ~24 states serving 7.4 million members
ABA Medicaid Exposure: ~10,000 children with ASD receiving ABA through UHC Medicaid plans; ~$290 million projected Medicaid ABA spend (2024); 20% year-over-year growth in utilization
Key Revelation: December 2024 ProPublica investigation based on leaked Optum internal documents detailing cost-containment playbook for ABA services
Internal Strategy: Rigorous utilization management; approach to authorizing fewer units than requested; provider network contraction (40%+ in some states); flagging providers for “outlier patterns”
Impact on Clients: Up to 19% of current ABA clients could see hours reduced or eliminated; Medicaid provider networks contracted in multiple states
Target States: Arizona, Nebraska, Tennessee, Virginia, New Jersey, Indiana, Louisiana (states with highest Medicaid ABA costs)
Louisiana Exit: Louisiana did not renew UHC Medicaid contract; 330,000 members reassigned by April 2026; state alleged contract violations re: prescription drug pricing
Public Commitments: Pledged to reduce prior auth requirements by 10% in 2025; part of 50+ insurer June 2025 PA reform pledge; Gold Card program for qualifying providers
Denial Rate: 9.1% Medicare Advantage PA denial rate (2023, above industry average); 85.2% appeal overturn rate
Parity History: $15.6M settlement for parity violations (2021); Wit v. UBH found defective review criteria affecting 50,000+ individuals; Delaware $450K parity penalties (2025)
DOJ Investigation: Criminal and civil probes into Medicare billing practices confirmed July 2025; expanded to Optum Rx and physician reimbursement; FBI and HHS OIG involved
Corporate Upheaval: CEO Brian Thompson killed Dec. 4, 2024; CEO Andrew Witty resigned May 2025; 2025 guidance suspended; stock down 42%+; former CEO Stephen Hemsley returned
Key Clinical Criteria: Optum references CASP practice guidelines, which state no specific limit on duration of ABA treatment; requires measurable progress on norm-based assessments every 3 months
Authorization Process: Two-step: assessment authorization (10–15 hrs), then treatment authorization; reauthorization required every several months with progress data
MUE Concerns: Payers misapplying Medically Unlikely Edits as daily hour caps on ABA; ABA Coding Coalition and CASP urge providers to bill beyond MUEs and appeal all denials
Parity Act: Mental Health Parity and Addiction Equity Act (2008) prohibits differential treatment of behavioral health vs. medical/surgical benefits
EPSDT Protection: Federal law requires Medicaid to cover all medically necessary services for children under 21; no hard hour caps permitted
Family Rights: Appeal denied/reduced authorizations (180 days commercial, 65 days MA); Medicaid fair hearing + aid pending for Medicaid members; file parity complaints with state insurance commissioner or DOL
Key Advocacy Orgs: Autism Speaks; Council of Autism Service Providers (CASP); Autism Legal Resource Center; Mental Health and Autism Insurance Project; National Health Law Program; ABA Coding Coalition
SOURCES & REFERENCES
Investigation: ProPublica, “UnitedHealth Is Strategically Limiting Access to Critical Treatment for Kids With Autism,” December 13, 2024 (Annie Waldman)
Company Financials: UnitedHealth Group 2024 and 2025 annual reports; SEC filings (Q4 2024, Q3 2025); Becker’s Payer Issues
Clinical Criteria: Optum ABA Supplemental Clinical Criteria (2025); UnitedHealthcare Community Plan Level of Care Guidelines — ABA (Tennessee); CASP Practice Guidelines (2014, reaffirmed 2020)
Provider Network: Optum Provider Express, “Our Network” page (providerexpress.com); Medicaid ABA network restrictions confirmed as of 2026
Louisiana Exit: Louisiana Department of Health announcement, December 12, 2025; Louisiana Illuminator reporting, December 2025; Access Health Louisiana, January 2026
MUE Analysis: Kornack, Unumb & Williams, “Preventing Insurance Denials of ABA Treatment Based on Misuse of MUEs,” Behavior Analysis in Practice (2023); ABA Coding Coalition; CASP MUE toolkit
Parity Settlement: U.S. DOL and NY AG v. United Healthcare Insurance Co. et al. (August 2021; $15.6M); Delaware DOI (September 2025; $450K)
Wit v. UBH: Wit v. United Behavioral Health, N.D. Cal. (2019 liability ruling; 50,000+ affected individuals)
DOJ Investigation: Wall Street Journal (February, May, July 2025); Bloomberg (August 2025); UHG SEC filing (July 24, 2025); CNBC, CNN, Fierce Healthcare reporting
PA Reform Pledge: AHIP / CMS insurer commitment (June 2025); Becker’s (April 2025); MedCity News (December 2025)
PA Denial Data: UHC 9.1% MA denial rate and 85.2% appeal overturn rate: CMS Medicare Advantage data (2023); Muni Health analysis
Federal Law: Mental Health Parity and Addiction Equity Act (P.L. 110-343, 2008); EPSDT: Social Security Act §§1902(a)(43), 1905(a)(4)(B), 1905(r)
Published: BreakingNewsABA.com — March 2026