The Hype vs. the Reality
The ABA technology landscape is saturated with AI claims. Search for “AI ABA software” and every company on the first page of results describes itself as AI-powered. But there is an enormous difference between software that uses a rules-based algorithm to auto-populate a scheduling template and software that deploys a trained machine learning model to generate clinical session notes from raw behavioral data. The first is automation. The second is AI. Both are useful. Only one justifies the label.
The distinction matters because ABA is at a crossroads. The industry faces simultaneous crises in documentation burden, billing compliance, workforce burnout, and outcomes measurement. Clinicians spend an estimated 30 to 40 percent of their working time on non-billable administrative tasks — writing session notes, generating progress reports, updating treatment plans, and managing authorizations. AI tools that can genuinely reduce that burden without compromising clinical accuracy represent a meaningful advance. Tools that simply rename existing features as “AI-powered” waste everyone’s time and erode trust in a technology that the field desperately needs to adopt thoughtfully.
What follows is an assessment of five companies that have shipped real AI features into production — tools that are being used by clinicians today, not prototypes or roadmap items. For each, we describe what the AI actually does, what data it trains on, and what the limitations are.
1. CentralReach: cari™ — The Industry’s Largest Proprietary AI
CentralReach is the dominant enterprise practice-management platform in ABA, serving multi-site providers and large organizations. In 2023, the company announced cari™ — a generative AI assistant built on what CentralReach describes as the largest proprietary dataset in autism and IDD care. Unlike generic AI tools that train on public internet data, cari is trained specifically on ABA clinical data within CentralReach’s HIPAA-compliant, proprietary LLM environment.
What it actually does: Automated session note generation from collected session data. Assessment recommendation engine that suggests evaluation tools based on client profiles. Scheduling optimization that recommends staffing configurations. Clinical test prep support for BCBA certification candidates. Revenue cycle management insights including denial prediction and claims optimization.
What makes it different: Scale and data. CentralReach processes data from thousands of ABA providers and hundreds of thousands of clients. The model is trained by a team that includes BCBA-D clinicians and subject matter experts who validate outputs. CEO Chris Sullens has emphasized that the AI is not designed to replace clinicians but to reduce time spent on non-reimbursable tasks.
Limitations: Enterprise pricing puts CentralReach beyond the reach of small and solo practices. The AI’s recommendations require clinical review and approval — it is a decision-support tool, not an autonomous system. The proprietary LLM approach means the model’s training data and reasoning are not publicly auditable.
2. RethinkBH: Session Note AI — Documentation at Scale
RethinkBH (formerly RethinkFirst) has deployed Session Note AI as a dedicated feature within its platform. The tool is designed to solve what is arguably the single biggest administrative pain point in ABA: writing session notes. BCBA supervision notes and RBT session documentation are required for billing compliance and clinical accountability, but they consume enormous amounts of non-billable time.
What it actually does: Generates HIPAA-compliant, audit-ready session summaries from data collected during therapy sessions. The AI pulls from session data — targets addressed, client responses, behavior incidents, and intervention types — to produce narrative documentation that meets payer requirements. Notes can be customized by length, focus area, and clinical emphasis.
What makes it different: RethinkBH has a large installed base of enterprise ABA providers and a library of over 1,500 pre-built treatment goals that provide structured clinical context for note generation. The company’s curriculum library means the AI is generating notes within a clinically defined framework, not from open-ended prompts.
Limitations: AI-generated notes must be reviewed and signed by the treating clinician. The tool assists documentation but does not eliminate the clinician’s responsibility for accuracy. There is an inherent tension between AI efficiency and the clinical purpose of note-writing: if the note becomes a rubber-stamp exercise, the documentation loses its value as a clinical reflection tool.
3. Hi Rasmus: Voice-to-Clinical-Text — The Multilingual Play
Hi Rasmus operates in a different market segment than CentralReach or RethinkBH. The platform serves providers across 60 countries, working with payer models that range from private pay to insurance to government funding. Its AI features are designed for global clinical workflows where documentation standards vary significantly.
What it actually does: Voice-to-text functionality that goes beyond basic transcription — the system processes and cleans natural speech patterns into professional clinical narratives. Automatic identification and pre-selection of intervention types based on the programs used during a session. AI-generated comprehensive session summaries based on collected data, with customizable parameters for length, focus areas, and excluded programs. Cross-language content conversion for family communication.
What makes it different: The multilingual capability is unique in the ABA software market. A clinician can narrate session observations in English and the system can produce a summary for a Spanish-speaking family. The voice-to-clinical-text pipeline is more sophisticated than standard dictation — it interprets clinical intent, not just words. Built-in verification requirements ensure clinicians review and confirm AI-generated content before finalizing.
Limitations: The 60-country footprint means the platform must accommodate regulatory frameworks that differ dramatically from U.S. payer requirements. Features optimized for international markets may not map perfectly to U.S. Medicaid or commercial insurance documentation standards. The company’s market presence in the U.S. is smaller than CentralReach or RethinkBH.
4. Raven Health: AI Session Summaries for Small Practices
Raven Health occupies a different niche: mobile-first, startup-friendly ABA software designed for new and growing practices that need simplicity, fast onboarding, and integrated data-collection-to-billing workflows. The platform’s AI features are targeted at reducing documentation time for clinicians who may be managing their own billing and administration.
What it actually does: AI-generated session summaries that synthesize collected behavioral data into progress narratives. The system analyzes skill acquisition data and behavior reduction metrics to produce summaries that can be shared with families or submitted to payers. Interactive progress graphs with real-time analytics allow clinicians to visualize trends without manual data manipulation.
What makes it different: Accessibility. Raven’s pricing and onboarding are designed for solo BCBAs and small clinics — the company claims BCBAs can learn the system in under an hour and RBTs in 15 minutes. Offline data collection with automatic sync means the AI features work for in-home and school-based providers who may not have reliable internet. The platform brings AI-assisted documentation to the segment of the market that enterprise platforms don’t serve.
Limitations: The AI capabilities are narrower than enterprise platforms — focused on session summaries and progress visualization rather than scheduling optimization, assessment recommendations, or denial prediction. Small-practice focus means the model trains on less data than CentralReach’s proprietary dataset. Practices that outgrow Raven may need to migrate to a more full-featured platform.
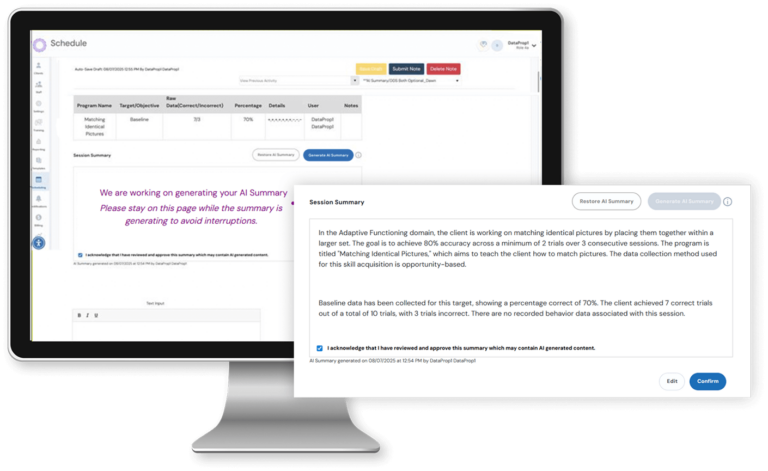
5. Ensora (formerly Catalyst by DataFinch): Real-Time Clinical Dashboards
Ensora ABA, formerly known as Catalyst by DataFinch Technologies, has been a staple of the ABA data-collection market for years, known for its fast, therapist-friendly mobile data entry and offline support. The platform has evolved to include AI-enhanced clinical dashboards and fidelity monitoring tools.
What it actually does: Real-time clinical dashboards that flag clients at risk of plateau or regression, prompting timely intervention by the supervising BCBA. Fidelity checks that monitor program adherence and staff performance across sessions. Predictive analytics that identify behavioral trends before they become clinically significant, enabling proactive treatment plan adjustments.
What makes it different: Ensora’s strength is in clinical data integrity. The platform emphasizes treatment classification accuracy and consistent implementation across therapists. Its AI features are oriented toward clinical decision support rather than administrative automation — helping BCBAs make better treatment decisions, not just write faster notes.
Limitations: The platform has historically had fewer enterprise billing and scheduling features than competitors like CentralReach, though it has been expanding its capabilities. The clinical-decision-support orientation means the AI is less visible to administrators and more embedded in clinical workflows, which can make it harder for practice owners to quantify ROI.
“Not every platform that mentions ‘AI’ actually delivers. Ask about automated session notes, denial prediction, and adaptive individualized care planning. True AI software should integrate seamlessly into your daily workflows, not sit on the sidelines.” — Raven Health, AI feature guide
What AI Cannot Do — and the Risks of Pretending It Can

The five companies profiled above represent genuine AI deployment in ABA. But it is equally important to understand what AI cannot do in 2026 — and the risks that arise when the technology is oversold.
AI cannot determine medical necessity. Whether a child needs 30 hours of ABA per week or 15 is a clinical judgment that depends on assessment data, family context, co-occurring conditions, and treatment history. An AI model can organize and present that data, but the decision is the BCBA’s.
AI cannot replace supervision. The BACB’s ethical requirements for supervision exist because clinical quality depends on human observation, feedback, and judgment. An AI that generates a session note does not observe whether the RBT implemented the protocol correctly. That remains a human responsibility.
AI cannot guarantee billing compliance. AI-generated session notes that are signed without meaningful clinician review create audit risk. If an OIG auditor finds that notes across hundreds of sessions read identically because they were auto-generated from templates, the documentation may be deemed insufficient regardless of whether the services were actually provided. The documentation must reflect what actually happened in the session, not what the AI infers should have happened.
AI cannot measure outcomes. The ABA industry’s existential challenge — proving that therapy produces measurable results — requires not just data collection but data interpretation, standardized outcome definitions, and longitudinal analysis that current AI tools are not designed to perform. AI can assist with data aggregation and trend identification, but the outcomes measurement framework must be built by clinicians and researchers, not algorithms.
The companies that are honest about these limitations — that describe their tools as decision support rather than autonomous systems, that require clinical review of AI outputs, that invest in BCBA-led model training rather than generic LLMs — are the ones most likely to build lasting value. The ones that oversell will contribute to the backlash that inevitably follows when a technology fails to deliver on inflated promises.
AT A GLANCE
Company 1: CentralReach — cari™: Generative AI on largest proprietary ABA dataset; session notes, assessment recommendations, scheduling optimization, denial prediction; HIPAA-compliant proprietary LLM; BCBA-D-trained; enterprise pricing
Company 2: RethinkBH — Session Note AI: Automated audit-ready session summaries from collected data; 1,500+ pre-built treatment goals as context framework; enterprise ABA providers; customizable note parameters
Company 3: Hi Rasmus — Voice-to-Clinical-Text: Speech-to-professional-narrative AI; multilingual translation for family communication; auto-identifies intervention types; 60-country deployment; built-in clinical verification requirements
Company 4: Raven Health — AI Session Summaries: Mobile-first platform for small/growing practices; AI-generated progress narratives from behavioral data; offline data collection with sync; BCBA onboarding in <1 hour; accessible pricing
Company 5: Ensora (formerly Catalyst/DataFinch) — Real-Time Dashboards: Clinical decision support; flags plateau/regression risk; fidelity monitoring; predictive behavioral trend analysis; therapist-friendly mobile data entry
Common AI Uses: Session note generation; progress report automation; scheduling optimization; behavioral trend identification; denial prediction; assessment recommendation; fidelity monitoring
Not Yet AI-Ready: Medical necessity determination; supervision replacement; autonomous treatment planning; outcomes measurement; billing compliance without human review
BACB Position: No specific AI-use guidelines issued as of early 2026; practitioners bound by Ethics Code (data privacy, informed consent, evidence-based practice); any AI tool must be evaluated against ethical standards
Admin Time Savings: Clinicians spend ~30–40% of working time on non-billable tasks; AI platforms report reducing administrative tasks by up to 40%
Market Context: U.S. ABA market ~$7.97B (2025), projected $9.96B by 2030; 132,307 BCBA job postings (2025); AI-driven efficiency is workforce retention strategy, not just productivity tool
Data Accuracy: AI treatment classification accuracy ~89.5%; predictive models achieving AUROC ~0.895; voice-to-text requires clinical cleanup; all outputs require human verification
Key Risk: AI-generated documentation that is signed without meaningful review creates OIG audit exposure; identical AI-produced notes across sessions may be flagged as insufficient documentation
Ethical Concern: If note-writing becomes rubber-stamp exercise, documentation loses clinical reflection value; AI must support clinical thinking, not replace it
Investment Trend: CentralReach (Insight Partners-backed); RethinkBH (enterprise SaaS); Raven Health (startup growth); all investing in AI as competitive differentiator and retention tool
SOURCES & REFERENCES
CentralReach: centralreach.com; cari™ announcement (2023); CR Unite presentations; CEO Chris Sullens statements
RethinkBH: rethinkbehavioralhealth.com; Session Note AI product page; 1,500+ treatment goal library
Hi Rasmus: hirasmus.com; AI-Powered Session Notes feature documentation (December 2024); 60-country deployment data
Raven Health: ravenhealth.com; AI session summaries feature; GetApp/SoftwareAdvice reviews; pricing documentation
Ensora/Catalyst: ensorahealth.com; clinical dashboard and fidelity monitoring features; DataFinch Technologies heritage
Industry Data: BACB Employment Demand 2010–2025; BLS projections; ABA Matrix Trends 2026; VG Soft Co ABA News (May 2025); Applied Behavior Analysis EDU AI integration guide
AI Accuracy: Treatment classification ~89.5% accuracy; AUROC ~0.895 (VG Soft Co, May 2025); administrative task reduction up to 40%
Published: BreakingNewsABA.com — March 2026